

Recent advances in 3D bioprinting for cartilage and osteochondral regeneration

Cartilage and osteochondral tissues are vital tissues in the human body for normal activities. Cartilage and osteochondral defects represent prevalent clinical entities due to the limited regenerative capacity of the corresponding tissues. This growing disease burden underscores the urgent need for advanced therapeutic strategies facilitating both cartilage and osteochondral regeneration. With advancements in bioprinting technology, cartilage and osteochondral tissue engineering offers new hope for treatment. However, bioprinting of cartilage and osteochondral tissue still faces significant challenges, including replicating the mechanical properties and lubrication function of cartilage and osteochondral tissue, as well as mimicking the structural complexity of bone–cartilage tissues. In recent years, the development of innovative bioinks and novel bioprinting technologies has provided new solutions for the biomanufacturing of cartilage and osteochondral tissue. This article systematically reviews the latest developments in the field of bioprinting for cartilage and osteochondral tissue engineering, addressing potential directions, challenges, and covering topics, such as bioprinting techniques, bioinks, and recent advancements in cartilage and osteochondral regeneration. Through this article, future potential directions and existing challenges in the bioprinting of cartilage and osteochondral tissue can be further clarified.
1. Introduction
The field of regenerative medicine has made significant progress in recent years with the development of three-dimensional (3D) bioprinting technology1,2—an innovative approach that allows for the fabrication of complex biological structures with high precision and accuracy.3,4 One of the promising applications of 3D bioprinting is in the regeneration of cartilage and osteochondral tissue.5,6
Cartilage and osteochondral tissue are essential for the proper functioning of joints, but they have limited self-repair capabilities, making it challenging to treat injuries and diseases that affect these tissues.7 Traditional treatments for cartilage and osteochondral damage include joint replacement surgeries, which have several limitations, including long recovery times and potential complications.8–10
3D bioprinting offers a novel approach for the regeneration of cartilage and osteochondral tissue by providing a platform for the fabrication of custom-made scaffolds that mimic the native tissue’s structure and function.11 These scaffolds can be seeded with cells and growth factors to promote tissue regeneration, allowing for the creation of living tissues that can integrate with the surrounding tissue.3
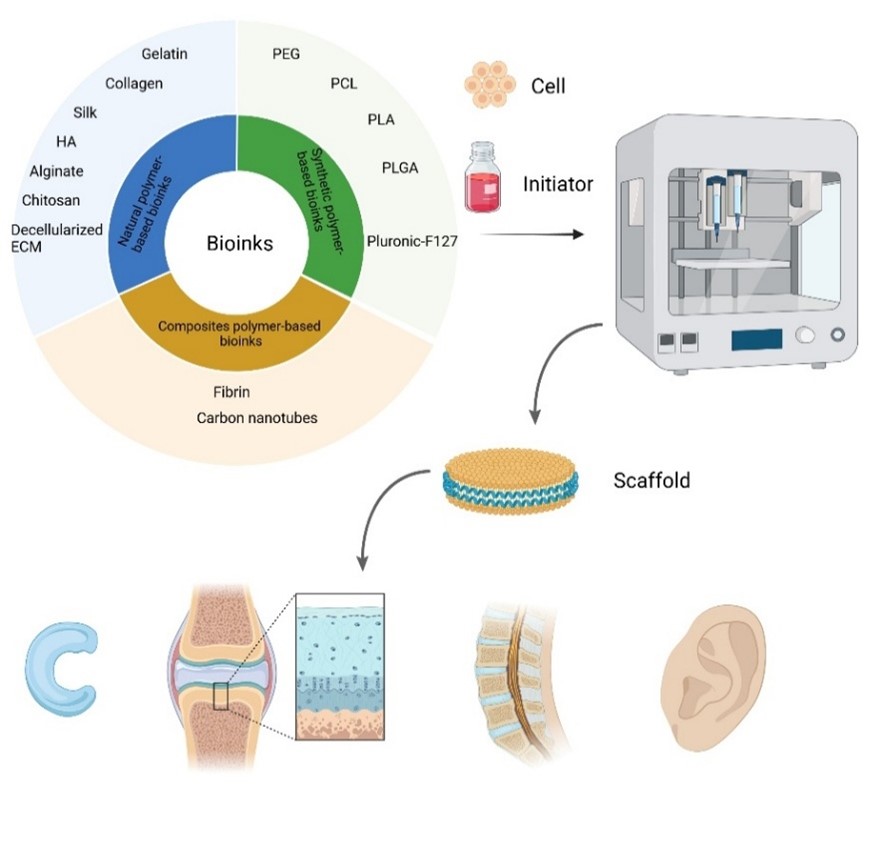
In this article, we explore the current state of 3D bioprinting technology for cartilage and osteochondral regeneration, including the various bioinks and techniques used in the fabrication of scaffolds and the challenges that must be addressed to translate this technology into clinical practice (Figure 1).

Figure 1. Overview of 3D bioprinting for cartilage and osteochondral regeneration. Abbreviations: ECM: Extracellular matrix; HA: Hyaluronic acid; PCL: Polycaprolactone; PEG: Polyethylene glycol; PLA: Polylactic acid; PLGA: Poly lactic-co-glycolic acid.
2. 3D bioprinting strategies
2.1. Inkjet bioprinting
Inkjet printing technology is a printing technology in which ink is sprayed onto a substrate in a non-contact manner, capable of depositing any printable ink on any desired substrate while causing negligible damage to the substrate. Inkjet technology has revolutionized the way we print text and pictures and is widely used in electronic device manufacturing.12 Later, researchers realized that the contactless and on-demand drip properties of inkjet printing may facilitate accurate patterning of biomaterials without contamination and waste of ink. Inkjet printing can deliver a wide variety of different materials and cells to specific locations with precision in both a non-contact and on-demand manner, thus, having the possibility of constructing complex heterogeneous biomimetic structures required by researchers.12 In 3D bioprinting, the ink of inkjet printing is replaced by a cell containing bioink, and the paper of inkjet printing is switched to the x–y–z controllable platform in 3D bioprinting, which allows for the 3D fabrication of biologically relevant objects. Bioink deposition is based on the temporal deformation of the internal space inside the nozzle through which the bioink flows, due to piezoelectric excitation or digitized thermal excitation. This deformation allows the dispensing of liquid drop-by-drop onto the collection platform, and the main advantages of hierarchical structure inkjet bioprinting in the z-axis are the simplicity of the system and the relatively low cost.13 In the case of inkjet bioprinting, the bioink is dispensed using piezoelectric or thermal actuation, allowing for precise deposition of droplets of the bioink.14 Researchers have recognized that inkjet printing has the potential to precisely pattern biomaterials without contamination or ink waste.15 Inkjet bioprinting enables the simultaneous and accurate delivery of multiple different materials and cells to specific locations in a non-contact, on-demand manner, making it possible to construct complex heterogeneous biomimetic structures required by researchers.14 Additionally, the droplet size produced by inkjet printing is in the picoliter range, allowing for high-precision positioning of microscopic biological components in digital graphics.12 The nozzle diameter of inkjet devices is typically around 50 μm, which is similar in size to cells, making cell printing or even single-cell printing a possibility.12 Biomaterials for inkjet bioprinting need to have a lower viscosity compared to extrusion-based bioprinting. In addition, the fluid density and surface tension of these biomaterials also need to meet high requirements, which can hinder their flow and droplet formation. The viscosity of biomaterials used in inkjet printers ranges from 3 to 30 mPa·s, the surface tension ranges from 20 to 70 mJ·m-2, and the proposed density is 1000 kg·m-3.12 When printing cell-containing bioinks, the characteristics and endurance of cells need to be considered. For example, when using an MJ-ABL piezo inkjet nozzle (MicroFab) with a diameter of 120 μm to print biological solutions, the droplet frequency is 20–60 Hz. The self-built pneumatic valve-type microdroplet on-demand injection system can spray human peripheral blood lymphocytes and culture medium at a frequency of 20 Hz, which can ensure the survival rate of cells after the injection process is close to 100%. In other studies, when printing mammalian cells, the emission frequency is set to 50–200 Hz, and there are also settings of 5 Hz to obtain high-quality images.16
However, inkjet bioprinting does have some limitations, including the limited range of cell densities that can be used for bioprinting and the viscosity range of bioinks.17 During inkjet printing, cell viability is regarded as a function of pressure, inkjet-substrate distance, liquid viscosity, and percentage of substrate gelling. Hendriks et al.18 presented a comprehensive study of the key factors associated with cell viability during drop-based printing, which could provide a reference for optimizing cell viability in this field. Despite these limitations, inkjet technology has become a practical tool in modern medicine,19 drug discovery,20 and tissue engineering.5 Inkjet bioprinting has been successfully used to create various tissue-engineered structures, including bone and cartilage structures.21 In conclusion, inkjet bioprinting shows promise in the field of 3D bioprinting and will continue to be an area of active research and development.
2.2. Extrusion bioprinting
Extrusion-based 3D printing has become a popular technique for tissue engineering applications since its introduction in 2002 by Heinrich et al.3 Extrusion-based bioprinting can be seen as a step up from inkjet bioprinting, using pneumatic or mechanical transmission as the driving force, which continuously extrudes bioink from the nozzle and deposits bioink on the platform substrate to construct the 3D structure.22
Extrusion-based bioprinting possesses several advantages, including the capacity to deposit high-viscosity bioinks and large cell densities.8 Moreover, extrusion-based bioprinting systems can continuously extrude bioinks without interruptions, which is preferable in most applications, considering the requirement for the integrity of bioprinted tissue constructs.23 Compared to the single-droplet deposition of inkjet bioprinting, extrusion bioprinting with continuous deposition can construct more complete 3D tissue structures. By providing sufficient thrust through actuation methods, extrusion bioprinting is compatible with multiple types of biomaterials, supporting a wide viscosity range of bioinks (30 to >6 × 107 mPa·s) and high cell density (>108 cells/mL or cell pellets).3 To allow the material to be extruded, three solutions are currently employed in most extrusion-based bioprinting systems to deliver the necessary pressure force: (i) pneumatic system, (ii) screen-based system, and (iii) piston-based system.24 Pressure control in extrusion bioprinting can affect material extrusion, cell viability, as well as structural accuracy and quality. The relevant parameters of pressure control include: (i) Nozzle diameter: The smaller the nozzle diameter, the greater the pressure required to extruder the material. (ii) Material properties: The viscosity, elasticity, and other characteristics of the material affect the pressure control. High-viscosity materials require more pressure extrusion and are more sensitive to pressure changes. The pressure required for low-viscosity materials is small, but improper pressure control can easily lead to unstable extrusion volume. (iii) Printing speed: Printing speed and pressure are interrelated. To improve the printing speed, it is necessary to increase the pressure to ensure the timely extrusion of the material. Reducing the printing speed can reduce the pressure appropriately. Often, a compromise must be made between applying sufficient pressure to ensure extrusion and avoiding excessive pressure to prevent damage to living cells. Applying more pressure than required may lead to unstable material flow, while too low pressure may lead to discontinuities in the deposited material. The percentage of cell viability changed significantly due to the change in pressure, with a change in viability of up to 38.75% measured.25 However, the bioprinting speed is relatively slow to build up a 3D structure, and the resolution is strongly dependent on different components, such as the nozzle size. The resolution of extrusion bioprinting can be controlled through nozzle size, which limits the manufacturing accuracy of the constructed tissue. A smaller nozzle is linked to greater shear stress on the cells in the bioink during the printing process, which ultimately affects cell activity and leads to cell death.26
Although extrusion bioprinting has the drawbacks of low resolution and poor cell activity, it is still the most widely used bioprinting method in tissue engineering, which is attributed to its high throughput, low cost, compatibility, and versatility.2
2.3. Stereolithography and digital light processing-based printing
Stereolithography for additive manufacturing was first demonstrated in 1986 by Charles W. Hull.3 He described the process of creating 3D objects by selectively transforming the physical state of a fluid to a solid through layer-by-layer photocrosslinking.3 Stereolithography bioprinting, a light-based printing technology, patterns the photosensitive bioink onto a substrate through optical projection and solidifies it layer by layer to achieve 3D construction with complex structures. This method is effective in fabricating intricate constructs and has faster printing, higher resolution, and production speed compared to extrusion-based bioprinting methods.27,28 Stereolithography has higher accuracy and better repeatability compared to other printing methods because it has no nozzle structure, and no shear forces are applied to the material and cells during bioprinting. Tissue structures printed using this technique are able to maintain high cell viability (>85%), so stereolithography is commonly used to construct functional organs.3 Stereolithography results in no shear stress to cells, allowing for high cell viability.3 It enables rapid bioprinting of structures without applying shear forces to the cells and with high resolution (± 1 μm).29 It is worth noting that in this printing technology, we need to control the light source parameters, printing material parameters, printing layer thickness, printing speed, and platform motion accuracy to ensure its advantage of high precision. To control the light source, various relevant parameters need to be investigated further: (i) Wavelength: The common wavelengths are 365, 405, and 780 nm. 365 and 405 nm belong to the ultraviolet (UV) and blue light range and can effectively excite most photopolymerization reactions. (ii) Intensity: The intensity of the light source is generally about 10–30 mW/cm². At this strength, the entire layer can be cured at one time by photographic means, allowing the structure to be crosslinked 50 times faster than other printing methods while maintaining cell viability. Too high a strength may damage cells, but too low a strength may result in incomplete curing. (iii) Exposure time: The exposure time is usually between 1 and 10 s. For specific bioinks and cell types, experiments are needed to determine the optimal exposure time. A short exposure time may not provide enough energy to fully cure the resin, affecting the structural strength. Longer exposure times may have adverse effects on the cells, such as decreased cell activity. Cartilage and meniscus have been successfully designed and developed using this technology.30 A major drawback of this system is that the liquid must be transparent with limited scattering; otherwise, light will not be able to pass through the material uniformly, resulting in non-uniform crosslinking. Because of this requirement, the cell density in the bioink was limited to ~108 cells/mL.13
3. Inks for 3D bioprinting of cartilage
3.1. Natural polymer-based bioinks
Bioinks used in 3D bioprinting for cartilage and osteochondral regeneration are generally divided into natural polymers, synthetic polymers, and composites. Natural bioinks generally refers to natural biomacromolecules extracted from natural sources (animals, plants, and microbes).
Natural bioinks can be classified by the major component, such as carbohydrate (agarose [Ag], alginate, chitosan, hyaluronic acid [HA]) or protein (gelatin, fibrin, silk)31 (Table 1).
Table 1. Overview of the characteristics and advantages of different bioinks
| Inks | Material category | Structure | Diameter of the ink raw material particles | Young’s modulus | Key advantage | Ref. |
|---|---|---|---|---|---|---|
| Gelatin | Natural protein | Thermoresponsive hydrogel | 30–300 nm | 10–100 kPa | Excellent cell adhesion | 44,45 |
| Collagen | Natural protein | Fibrous ECM-mimetic network | 50–200 nm | 5-–5 kPa | Native ECM composition | 34,36 |
| Silk | Natural protein | β-sheet crystalline network | 10–30 μm | 1–5 MPa | High tensile strength | 55,138 |
| HA | Natural glycosaminoglycan | Viscoelastic hydrogel | 50–200 nm | 2–20 kPa | Chondrocyte differentiation promoter | 58,139 |
| Alginate | Natural polysaccharide | Ionically crosslinked microbeads | 200–800 μm | 20–100 kPa | Ionic crosslinking control | 63,140 |
| Chitosan | Natural polysaccharide | pH-sensitive porous scaffold | 50–300 μm | 50–500 kPa | Antimicrobial properties | 66,141 |
| dECM-based | Natural composite | Native ECM-derived fibrillar scaffold | 100–500 μm | 5–50 kPa | Preserved bioactive factors | 70,142 |
| Fibrin | Natural polymer | 3D fibrin clot matrix | 40–250 nm | 15–50 kPa | Rapid polymerization | 81,82 |
| PEG | Synthetic polymer | Photocrosslinked hydrogel network | 10–50 nm | 50–1000 kPa | Tunable mechanical properties | 102,143 |
| PCL | Synthetic polyester | Melt-electrospun microfiber | 10–100 μm | 2–20 MPa | Slow degradation rate | 106,144 |
| PLA | Synthetic polyester | 3D-printed lattice structure | 100–300 μm | 1–3 GPa | High stiffness | 107,145 |
| PLGA | Synthetic copolymer | Nanoparticle-embedded matrix | 0.1–10 μm | 50–200 MPa | Controlled degradation | 109,146 |
| Pluronic F-127 | Thermoresponsive polymer | Thermoreversible micellar assembly | 20–50 nm | 1–10 kPa | Temporary sacrificial material | 111,147 |
| Carbon nanotubes | Nanomaterial additive | Nanofiber-reinforced composite | 5–20 nm | 1–10 GPa | Electrical conductivity enhancement | 114,148 |
| Cellulose nanocrystals | Nanomaterial additive | Usually rod composed of cellulose molecular chains | 0.1–10 nm | Prepared nanocellulose film can reach 57.8 GPa | High strength, high modulus, high crystallinity, and also have good optical, rheological, and biological activities | 132 |
| Halloysite nanotubes | Nanomaterial additive | Hollow tubular structure, composed of alternating silicon | 20–100 nm | 20–30 GPa | Large specific surface area, strong adsorption performance, easy to modify the surface, and can be functionalized to meet different application requirements | 134 |
Abbreviations: dECM: Decellularized extracellular matrix; ECM: Extracellular matrix; HA: Hyaluronic acid; PLA: Polylactic acid; PLGA: Poly lactic-co-glycolic acid; PCL: Polycaprolactone; PEG: Polyethylene glycol.
3.1.1. Collagen
The bioinspired scaffolds printed with collagen-based bioink mimic the natural cartilage structure and perform well in cartilage tissue repair and regeneration.32 Collagen is the major structural protein in the mammalian extracellular matrix (ECM). Collagen organizes itself into highly ordered 3D networks to support cell behavior and tissue functions. To date, a comprehensive understanding of human tissues and organs has yielded 28 different types of collagen, of which types I, II, III, and V constitute the major ECM components of various structures including cartilage, skin, tendon, bone, muscle, and cartilage.32,33 The hyaline cartilage in the joint is mainly composed of type II collagen. In native cartilage, the fiber network formed by collagen constructs the structural framework of the ECM of articular cartilage, and the distribution and orientation of collagen fibers provide the unique mechanical properties of articular cartilage.34 It is noteworthy that collagen is most stable at pH 7–7.2 and retains its native structure, supporting biological activity and cellular interactions in this pH range. Some 3D printing processes dissolve collagen under acidic conditions (pH 3–4) to maintain it in solution and neutralize it to physiological levels after printing to promote gelation and biocompatibility. Therefore, the pH and temperature must be carefully regulated during printing and ink preparation before using collagen as a bioink.35 In bioprinting, collagen can participate in cell activities and has superior biological characteristics. Collagen-based cartilage scaffolds can enhance the expression of cartilage growth factors, promote cartilage regeneration, and effectively reduce the risk of immune rejection of engineered cartilage.34,36 Bosnakovski et al.37 demonstrated that type II collagen, even without the use of growth factors to induce seed cell differentiation, has the potential to induce and maintain bone marrow mesenchymal stem cell chondrogenesis and interact with transforming growth factor beta (TGF-β)1 to enhance differentiation. However, the rapid degradation rate and poor mechanical properties of collagen limit its application in bone and cartilage tissue engineering. The main challenge in printing collagen is the inability to form structurally stable collagen structures under original conditions.38 Diamantides et al.39 used a blue-light-activated mixture of riboflavin with collagen to improve the mechanical properties of printed collagen while employing various printing strategies to form collagen-based structures with printing fidelity. Beketov et al.40 used a bioink with a high concentration of collagen (4 wt%) and chondrocytes for extrusion-based bioprinting for biomanufacturing. Ultimately, the resulting cartilage tissue has a unique structure with a syngeneic cell population and a high content of glycosaminoglycans (GAGs) and type II collagen. By integrating inkjet printing and electrospinning techniques, Jiang et al.41 created hybrid structures characterized by alternating layers of chondrocyte-loaded collagen-fibrin hydrogel and polycaprolactone (PCL) nanofibers. The compressive modulus and ultimate tensile strength of the hybrid scaffold were observed to be 1.76 and 1.1 MPa, respectively, which are much higher than the collagen-fibrin scaffold. Rhee et al.42 investigated the effect of different collagen concentrations in hydrogels on 3D bioprinting of cartilage tissue scaffolds. Alginate and temperature regulation were used during bioprinting to improve the gelling ability and printability of the collagen bioink. They noted that bioinks with collagen concentrations in the range of 12.5–17.5 mg/mL maintained a strong similarity to their original structures; however, the concentration of collagen had no apparent effect on cell survival, and the compressive strength was linearly related to the collagen concentration. This study highlights the potential of using high concentrations of collagen. High-density collagen is used to create scaffolds with excellent shape accuracy and mechanical properties for cartilage tissue repair purposes. Shim et al.43 used HA and atelocollagen to fabricate a multilayer scaffold. In osteochondral defects produced in the rabbit knee joint, the scaffold demonstrated the generation of new cartilage tissue. In addition, the newly produced cartilage is surprisingly intertwined with the cartilaginous tissue of the host. In addition, the marker proteins of cartilage, type I and II collagen, were expressed in the tissue, confirming cartilage formation in the resulting defects.43
3.1.2. Gelatin
Gelatin is a natural polymer produced by the hydrolysis of collagen. The advantages of gelatin are to provide good biocompatibility, solubility, and degradability. It can make the viscosity of bioink suitable for extrusion-based 3D bioprinting by changing the temperature or concentration of gelatin and thus, changing the viscosity of gelatin-based bioink.44 The thermal sensitivity of gelatin allows it to form hydrogels upon cooling at 20–30 °C, an indication that its bonds are easily broken by heat, enabling printing and stacking on itself in a controlled manner.45 For bioprinting applications, gelatin with a wide range of concentrations has been used as a bioink material or as a composite with other polymers. In addition, the rapid gelation property of gelatin, when it is bioprinted in 3D, can lead to its strong initial stability.46 Unmodified gelatin requires chemical reactions or the addition of other components (alginate, chitosan, fibrinogen, HA) to stimulate crosslinking. Gelatin is usually limited in bioprinting due to its poor mechanical properties. However, once gelatin is added with alginate, silk fibroin, chitosan, or other natural polymers, interactions, such as covalent bonds, hydrogen bonds, and van der Waals forces are enhanced, resulting in superior mechanical, functional, and biocompatibility over the same gelatin hydrogel.47,48 Sathish et al.47 reported the optimization of a composite, bioactive, and biocompatible trimeric hydrogel bioink with gelatin, carboxymethyl cellulose, and alginate as materials with optimized printing properties, structural properties, biomechanical properties, and biological functional properties for direct and indirect printing of customizable scaffolds for cartilage tissue engineering applications. Wang et al.49 used a (biological) ink pre-polymer consisting of sodium alginate (SA) and gelatin crosslinked by calcium chloride and microbial transglutaminase, respectively, to generate a double-network hydrogel with excellent mechanical properties and good biocompatibility. He et al.50 achieved enhanced printability and higher fidelity in extrusion bioprinting by sequential chemical modification of gelatin with reversible quadruple-hydrogen-bonded ureido-pyrimidinone (UPy) and enzyme-responsive tyramine moieties (Tyr) to provide temperature-programmable viscosity and enzyme-controlled solidification. Using modified gelatin to construct a variety of cell-loaded scaffolds, they demonstrated that Gel-UPy-TyR-based constructs could not only maintain high fidelity but also support the growth and function of loaded cells at physiological temperatures. Promising results were obtained when arginine–glycine– aspartic acid (RGD) was conjugated with natural polymers, such as gelatin. Researchers have shown that functionalized gelatin–RGD enhances the homing of mesenchymal stem cells (MSCs) cells into gelatin–RGD hydrogels and promotes faster tissue regeneration with new bone tissue and blood vessel formation in vivo compared to gelatin hydrogels.51 The binding of RGD to integrin receptors plays a major role in the cell adhesion mechanism. Souza et al.52 demonstrated increased cell growth and more extensive matrix colonization in alginate–gelatin–RGD hydrogels compared to alginate–gelatin hydrogels. During 3D printing, RGD molecules were added to a pre-determined portion of the alginate–gelatin matrix using a liquid-phase approach to promote cellular compartmentalization. In addition to being a printable bioink, gelatin viscoelastic can also serve as a support bath to allow gel-in-gel bioprinting of soft and low-viscosity bioinks while providing an environment that maintains cell viability.53 Gelatin is ideal for supporting the bath because the syringe needle can be easily inserted and passed through to extrude the bioink. As the needle moves forward, the gelatin solidifies in its wake and keeps the extruded material in place. In addition, the heat-gelatin responsiveness makes it easy to wash off the bath and recover the bioprinting structure.44 Kupfer et al.54 used gelatin microspheres to support the bioprinting of cardiac chambers utilizing a low-viscosity gelatin methacryloyl (GelMA). They printed a human-induced pluripotent stem cell-loaded construct with two compartments and a vascular inlet and outlet. After human induced pluripotent stem cells proliferated to a sufficient density, cells within the structure were differentiated, and the function of the resulting human compartment muscle pump was demonstrated. The human compartment muscle pump exhibits macroscopic beating and continuous action potential propagation that responds to drugs and pacing. The connected chambers allow perfusion and are able to replicate the pressure/volume relationship.
3.1.3. Silk
Silk has been widely used in tissue engineering because of its mechanical properties, biocompatibility, and controlled degradability. Its shear dilution properties make it an ideal material for extrusion bioprinting. Moreover, it can be physically crosslinked.55 Thus, eliminating the need for the use of harsh crosslinking chemicals. However, it has low viscosity, leading to the possibility of clogging on printing.56 Schacht et al.57 found that cell-loaded spider silk structures could be printed by robotic dispensing without the need for crosslinking additives or thickeners for mechanical stabilization. The cells could adhere and proliferate on the spider silk scaffold for at least 1 week. The introduction of cell-binding motifs into spider silk proteins further enables fine control of cell–material interactions.
3.1.4. Hyaluronic acid
HA is a non-sulfonated GAG that is widely distributed in human connective tissues.58 As one of the main components of natural cartilage like collagen, HA is often used as a material for cartilage defect repair. The advantages of HA are biocompatibility, biodegradability, high porosity, and easy maintenance of hydration.59 HA can affect the morphological changes of chondrocytes and promote the formation of new cartilage. However, HA itself is easily degraded in the biological environment and cannot maintain the stability of the scaffold structure for a long time. In addition, its low viscosity and poor molding properties limit its application in bioprinting.60 Hauptstein et al.60 developed an HA-based bioink composition. Thiolated HA and allyl-modified poly(glycinol) were crosslinked. Unmodified high-molecular-weight HA at the concentration of 1 wt%, was added. Improved ECM distribution in these structures was associated with increased structural stiffness after chondrogenic differentiation compared to structures with high concentrations (10 wt%) showing only pericellular matrix deposition. Wang et al.28 used digital light processing-based bioprinting simultaneously with structural fidelity, bioactivity, and high mechanical properties by using both photoactive bioinks, hyaluronic acid methacrylate (HAMA), and GelMA hybrid bioinks. In addition, they used hyaluronidase for post-enzymatic digestion of HAMA molecules, which required mechanical properties over a wide range (above 1 kPa to ~100 kPa), while the mechanical properties could be precisely regulated by the enzymatic digestion process. A library of mechanical properties related to biochain formulation and digestion parameters was further established by mathematical modeling. Gong et al.61 improved the resolution without the need to change any printer hardware or most of the bioink composition by post-shrinking the 3D-bioprinted structure. They chose HAMA as an anionic ink immersed in a polycationic chitosan solution for bioprinting. These printed structures were found to reduce their linear size to varying degrees by charge complexation and subsequent expulsion of water from the gel. Finally, they performed proof-of-concept studies using several 3D printing techniques, including direct extrusion printing, sacrifice printing, and microfluidic hollow fiber printing, and observed successful shrinkage in all cases. Antich et al.62 developed HA as a raw material, which conferred photocrosslinking ability through the methacrylic anhydride reaction to improve the printing fidelity and mechanical strength of HA scaffolds. HA-based bioinks were found to improve the functional chondrogenic gene marker expression and specific matrix deposition of the cells.62
3.1.5. Alginate
Alginate, a biocompatible anionic polymer extracted from brown algae, has been applied in tissue engineering due to its biocompatibility and relatively low cost.63 Alginate’s greatest advantage is that it can be used as a bioink by forming a hydrogel similar to the ECM.63 However, its low biological activity results in the inability to promote cell proliferation.64 Yang et al.65 used type I collagen or Ag mixed with SA, as a 3D bioprinting bioink and incorporated chondrocytes in vitro to construct 3D-printed cartilage tissue. The results showed that 3D-bioprinted SA/collagen had good mechanical strength and biological function, which was expected to be used in cartilage tissue engineering.
3.1.6. Chitosan
Chitosan is a natural polysaccharide made by the deacetylation of chitin. The advantages of chitosan are low toxicity, antibacterial properties, biodegradability, and biocompatibility.66 Lu et al.67 found that after the intra-articular injection of chitosan solution into the knee joint of rats, the chondrocytes were highly active and produced a large amount of ECM, and the density of newborn chondrocytes was also significantly increased. However, in bone and cartilage tissue engineering, its application is limited due to the relatively weak mechanical strength of chitosan.66 Huang et al.68 constructed a solid-supported thermogel consisting of a chitosan hydrogel system and a decalcified bone matrix. Composite biomaterials have better porosity, balanced swelling rate, and degradation rate compared to hydrogels or decalcified matrices alone.
3.1.7. Decellularized extracellular matrix-based bioinks
Decellularized extracellular matrix (dECM) can be obtained from decellularized tissue using a variety of physical and chemical methods, including freeze–thaw cycles, detergents, or enzymatic agents.69 It is ideal to provide cells with a natural microenvironment like their parent tissues. dECM is the best choice for doing so because no natural or man-made material can recapitulate all the features of natural ECM.70 Cartilage dECM is expected to stimulate chondrocytes to produce new cartilage dECM or chondrogenesis and has the potential to be incorporated into scaffolds with trizone structures for long-term weight bearing.71 The overall mechanical properties of cartilage dECM biomaterials were designed to achieve those of natural menisci, with Young’s modulus ranging from 72 to 132 MPa, compression modulus ranging from 100 to 400 kPa, and yield stress ranging from 12 to 21 MPa, with different local mechanical properties in different regions.72 Liu et al.73 prepared annulus fibrosus matrix (DAFM)/chitosan hybrid hydrogels. Annulus fibrosus (AF) stem cells were cultured on hydrogel scaffolds with or without basic fibroblast growth factor (bFGF). The results support the application of DAFM/chitosan hybrid hydrogels as suitable candidates for AF tissue engineering.
The umbilical cord consists of one vein, two arteries, and the surrounding myxomatous substance, which is called Wharton’s gum. Its ECM components contain a large amount of collagen, HA, and sulfated proteoglycans.74 Wharton jelly ECM is similar to cartilage ECM. It is also rich in peptide growth factors, including epidermal growth factor, platelet-derived growth factor, fibroblast growth factor (FGF), bFGF, insulin-like growth factor I (IGF-I), and TGF-β.75 These peptide growth factors contribute to the cellular biosynthesis of collagen and GAGs in cartilage formation, particularly IGF-I and TGF-β. Therefore, Wharton’s jelly ECM may be a good alternative biomaterial to tissue-engineered cartilage. Xiao et al.76 prepared Wharton’s jelly ECM scaffolds using waterproof crushing differential centrifugation combined with the freeze-drying method. The scaffolds have good biological activity and biocompatibility and have good application value in cartilage tissue engineering.
Natural bioinks have shown their ability to provide bioprinting structures with cellular structures and functional tissues. They have essential properties, such as biocompatibility, biodegradability, and high hydrophilicity.77 Natural biomaterials provide a favorable environment for cell growth by mimicking the natural ECM of tissues, self-assembling, and exhibiting biocompatible and biodegradable properties.78 However, natural bioinks form a non-covalent bond stable structure that cannot reach cartilage strength, and modification of the natural material is required to prepare bioinks. The composites prepared with 3D bioprinting technology can be widely used for cartilage tissue repair.62,79 Natural materials can be processed by physical, chemical, and protein self-assembly methods to achieve cartilage strength. The most used method at present is UV crosslinking based on methacrylic acid derivatives (GelMA, HAMA). Currently, the most used printing modality is still extrusion bioprinting, but a single bioink usually lacks sufficient biocompatibility and mechanical properties. Therefore, a mixture of two or more biomaterials is usually required.80
3.1.8. Fibrin
Fibrin is one of the natural biopolymers formed during blood coagulation, and it is a reticulated fibrous structure composed of a large number of random fibers.81,82 The internal regulation of fibrin by various means (Ca2+, pH, thrombin, etc.), such as fibril length, porosity, and density, allows for the control of the overall structural properties and enables the regulation of cell proliferation and differentiation.83 For example, Chiu et al.84 noted that an increase in fibrinogen concentration significantly reduces the pore size of fibrin gels and significantly decreases their permeability to nutrients, ultimately leading to insufficient nutrients being received by the cells inside the gel. As an ink for bioprinting, fibrin has unique mechanical properties; it is considered one of the softest polymeric fibers in nature, and the mechanics of fibrin can be tuned to a wide range, allowing a span of Young’s modulus from 0.1 to 5.5 kPa by adjusting the ratio of fibrinogen and thrombin concentrations.85 Fibrin can also be regulated by adding other biomaterials to fibrin, such as HA and gelatin. Snyder et al.86 increased the compressive modulus from 3.5 to 6.5 kPa with HAMA mixed with fibrin. Some groups also mixed fibrin and gelatin,87 and the mechanical elastic modulus of the composite hydrogels showed different performance at different mixing ratios, demonstrating the flexible mechanical property tuning ability of fibrin. Fibrin can also be used in the construction of stiffer tissues, and by combining fibrin with stiffer biomaterials, such as keratin88 and SA,89 a wide range of Young’s modulus changes (330–1700 kPa) can be achieved.88 Bioink composed of fibrin can be adapted to a variety of printing technologies, such as extrusion printing and injected printing.90 It should be noted that extrusion printing with fibrinogen alone as a bioink is difficult, and the printed scaffold has difficulty in maintaining the desired structure91 (Figure 2A).

Figure 2. Composite ink for cartilage 3D bioprinting. (A) Schematic diagram of fibrin ink printed in a PEG-alginate support bath. Reprinted with permission from ref.91 Copyright © 2019, Wiley-VCH. (B) Comparison of the effects of nano-hydroxyapatite and carbon nanotubes in promoting osteogenic differentiation of HASCs. Reprinted with permission from ref.123 Copyright © 2020, Elsevier Ltd. (C) Comparison of the differentiation effect of human ADSCs under PCL, graphene, and CNT (cells cultured for 21 days). Reprinted with permission from ref.124 Copyright © 2019, Elsevier Ltd. Abbreviations: ADSCs: Adipose-derived stem cells; HASCs: Human adipose-derived stem cells; PCL: Polycaprolactone; PEG: Polyethylene glycol; PEGDMA: Poly(ethylene glycol) dimethacrylate.
Due to its excellent mechanical properties and biocompatibility, fibrin has been used for the biomanufacturing of tissues, such as brain,92 cardiovascular tissue,93 skin,94 muscle tissue,95 nerve tissue,96 vessels,97etc. In cartilage tissue biomanufacturing, Melo et al.91 used fibrin-wrapped bone marrow mesenchymal stem cell (BMSC) spheres as bioink and printed in an interpenetrated network support bath composed of polyethylene glycol (PEG) and alginate. The results showed that MSCs could grow and differentiate in a soft environment and remain in a rigid support bath into cartilage differentiation due to the presence of fibrin.91 Kang et al.97 used PCL as a scaffold to provide mechanical properties and printed outer ear structures of the same size as the human ear using a hydrogel composed of gelatin/glycerol/fibronectin/HA loaded with chondrocytes (Figure 2B). The results showed that the cells survived well in the outer ear structure after printing, and new cartilage tissue could be observed inside the structure after 5 weeks of culture. The printed material was transplanted into subcutaneous cultures of mice and showed significantly elevated GAGs after 2 months, and no internal vascularity was generated as in native cartilage tissue. Moreover, the implanted tissue exhibited elasticity similar to that of the native rabbit ear.97 Because of its soft mechanical properties, fibrin is rarely used as a building block for hard tissues like bone. However, fibrin can act as a carrier for cells, and together with high-strength compositions (PCL and poly lactic-co-glycolic acid [PLGA]), it forms a scaffold for bone repair, ensuring cell viability while achieving mechanical strength.98
3.2. Synthetic polymer-based bioinks
The most significant advantage of synthetic bioink is controllable and can possess photocrosslinking ability. Meanwhile, its physical, chemical, and biological properties can be tuned.99 The strong mechanical properties of synthetic bioinks are attributed to their strong covalent bonds, aiding the bioprinting process and the shape retention of deposited structures. Compared with natural bioink, synthetic polymers exhibit more suitable mechanical properties and thus, are more capable of withstanding external pressure. Furthermore, they can support the development of porous structures and microchannels that help recapitulate the vasculature of native tissue.100 However, they are less biodegradable and biocompatible than natural bioink. In addition, synthetic polymers lack the bioactivity necessary to promote cell growth and proliferation and thus, are mainly used to provide structural support to the bioink101 (Table 1).
3.2.1. Polyethylene glycol
PEG is a synthetic polymer synthesized by ethylene oxide polymerization and has been widely used in 3D bioprinting for bone and osteochondral regeneration due to its strong mechanical properties and because it is not cytotoxic and immunogenic.102 It has been shown that the addition of PEG to the polylactic acid (PLA) solution not only promoted the scaffold printing process through its plasticizing effect but also led to structural and physicochemical changes in the resulting scaffolds.103 However, it is a bioinert material and cells cannot easily attach, so it needs to be combined with other bioactive hydrogels. Rutz et al.104 fabricated soft, printable gels from a variety of amine-containing polymers and polymer mixtures, both synthetic and natural, confirming that composites of PEG and natural biomaterials have been shown to improve the degradation properties of PEG-based structures.
3.2.2. Polycaprolactone
In the process of bioprinting, PCL microfibers were used to improve the mechanical properties of bioink. Mukherjee et al.105 used porous 3D-printed PCL and composite scaffolds to present similar and uniform degradation characteristics in vitro. Good tissue ingrowth was observed when GelMA-HAMA was combined with PCL. In a different study,106 using an extrusion-based bioprinting system in which PCL microfibers were incorporated into the bioink, the elastic modulus of alginate and GelMA bioink increased 544-fold and 45-fold, respectively; these values were in the range of articular cartilage. Cell viability studies showed that all the bioinks had a high level of MSC viability (about 80%) after bioprinting.
3.2.3. Polylactic acid
PLA has emerged as an important polymeric material for 3D bioprinting due to its biocompatibility, biodegradability, mechanical strength, and processing capability. It can be blended with different polymers to modify tissue-specific scaffolds.107 Ritz et al.108 confirmed the biocompatibility of PLA as well as endotoxin contamination levels below the U.S. Food and Drug Administration (FDA) limits. PLA-based 3D bioprint supports the growth, spreading, and proliferation of different cell types, such as osteoblasts, osteoblast-like cells, and human umbilical vein endothelial cells. Matrix-derived factor 1 (SDF-1) is released from the PLA cage, which supports the growth of endothelial cells and induces the formation of new blood vessels. These results demonstrated the potential of 3D-printed PLA scaffolds for bone tissue regeneration.
3.2.4. Poly lactic-co-glycolic acid
PLGA is usually synthesized by ring-opening copolymerization of lactic and glycolic acids, and its degradation products are non-toxic.109 Because PLGA has good biocompatibility, tunable degradability, and mechanical properties, PLGA-based 3D-printed scaffolds hold an important position in bone regeneration and repair. Human bone tissue is mainly composed of inorganic minerals and collagen fibers, which are usually modified using PGLA to accurately mimic the composition and structure of natural bone tissue.110
3.2.5. Pluronic-F127
Pluronic is a gel with good printing suitability and temperature sensitivity, ideal for use with bioink. Thus, Pluronic can be easily washed off after printing because it liquefies at 4°C or below.111 But due to insufficient biocompatibility to support long-term cell survival, it is not directly equivalent to bioprinting but rather requires conjugation with other polymers, such as acrylic acid.112 Madry et al.113 recently used Pluronic-F127 to guide the transfer of a recombinant adeno-associated virus gene vector into a miniature pig cartilage defect in vivo, promoting higher repair within 4 weeks than when transferred using a control group. Regarding the treatment of osteoarthritis lesions, Gun-Il Im 126 delivered the cartilage-protective molecule kartogenin using Pluronic-F127 nanospheres in a rat osteoarthritis model, which inhibited disease progression for at least 8 weeks relative to untreated animals.
3.3. Nanoparticles-based bioinks
3.3.1. Carbon nanotubes
Carbon nanotubes (CNTs) are graphene-based nanomaterials, which are formed by curling graphene sheets into cylinders, whereas CNTs formed by single-walled graphene sheets are single-walled carbon nanotubes (SWCNTs) with a diameter of about 0.5–2 nm, while those composed of multilayer graphene sheets are multiwalled carbon nanotubes (MWCNTs) with a diameter of up to 10–150 µm.114 The current methods for synthesizing CNTs are arc discharge, laser ablation, and chemical vapor deposition (CVD), and CNTs for biological applications are mainly prepared by the CVD method.115 Due to their excellent tissue compatibility and mechanical properties, CNTs have many applications in tissue regeneration and biofabrication. In bone tissue engineering, MWCNTs have shown excellent histocompatibility and tissue regeneration properties.116 When MWCNTs were implanted into the tibial defect of rats, the defect was completely restored after 4 weeks, and MWCNTs were incorporated into the bone marrow and bone matrix and tightly connected to the surrounding tissues.117 Additionally, MWCNTs showed unique cytokine delivery capability.118 For example, MWCNTs improved the ectopic ossification ability of the BMP-2/type I collagen composites, and the addition of MWCNTs resulted in a greater extent of ectopic ossification and more mineral content in the formed bone compared to the BMP-2/type I collagen composites alone group.117 Another advantage of MWCNTs is the mechanical properties, while its Young’s modulus can reach 1 TPa,119–121 the elastic modulus of cortical bone is 12–18 GPa, while the elastic modulus of cancellous bone is only 2–12 MPa.122 Therefore, MWCNTs can match the mechanical properties of normal bone tissue and achieve mechanical support in the area of bone defects. Du et al.123 examined the differences in osteogenic capacity between MWCNTs and nano-hydroxyapatite (nHA) (Figure 2B), which is the main inorganic component of bone tissue, and after inoculating human adipose-derived stem cells (HASCs) on CNT and nHA and culturing them for a period of time, there was no significant difference in the amount of cell adhesion on both, while the CNT group was significantly better than nHA in terms of adhesion effect. After 3 weeks of implantation of the two nanomaterials, abundant type I collagen tissue appeared around the CNT, while fibrous tissue appeared in the nHA group, and no significant enhancement of type I collagen immunostaining was seen, suggesting no bone tissue generation.123 In summary, CNTs show advantages in both cell adhesion and osteogenesis induction, and the strong mechanical properties of CNTs ensure that they can be used as bone defect repair materials matching the mechanical properties of bone tissue.
CNT can be added to bioink as an additive to confer its ability to promote osteogenic differentiation and chondrogenic differentiation. Wang et al.124 compared the differences between plain PCL scaffolds and PCL scaffolds with the addition of CNTs for biological applications. In terms of mechanical properties, the compressive modulus and compressive strength of PCL scaffolds were greatly improved with the addition of CNTs. In terms of protein adhesion and cell activity, the PCL scaffolds with the addition of CNTs were higher than the normal PCL scaffolds. When HASCs were seeded into PCL scaffolds incorporating CNTs and cultured for 21 days, calcium deposition was observed, showing potential in bone tissue repair124 (Figure 2C). Gonçalves et al.125 printed osteogenic scaffolds using HA, CNTs, and PCL as raw materials. The best combination of mechanical properties and electrical conductivity was exhibited at 2 wt% CNTs, and osteoblasts could perform normal cellular functions in the pores formed by the scaffold. Chahine et al.126 used modified CNTs for chondrocyte culture, and after grafting –COOH on SWCNTs, the secretion of cartilage ECM was significantly promoted. However, the mechanical strength of the scaffold differed from normal human cartilage tissue. CNTs also affect the proliferation and differentiation of stem cells. It has been shown that CNTs can promote the differentiation of BMSCs toward osteogenesis and the rate of differentiation is accelerated. However, in the presence of CNTs, the proliferation rate of BMSCs was decreased. Meanwhile, BMSCs attach to the CNT’s surface in a flat polygonal shape, which is considered one of the manifestations of BMSC differentiation toward osteogenesis and may be related to the surface microstructure of CNTs.127
An issue that should not be neglected regarding the application of CNTs is the toxicity. Impurities are inevitably produced during the production of CNTs, and due to the specificity of their structure, CNTs may produce effects similar to those of asbestos. The role of CNTs in pulmonary fibrosis has been pointed out,128 and CNTs may stimulate reactive oxygen species (ROS) production by macrophages, possibly due to intracellular degradation of CNTs.129 Therefore, how to circumvent the toxic effects of the use of CNTs is an issue that needs to be considered in the use of CNTs for biomanufacturing.
3.3.2. Cellulose nanocrystals
Cellulose nanocrystals (CNCs) are highly crystalline needle-like cellulose nanostructures of 10–20 nm in width and several hundred nanometers in length, flexible cellulose fibers with a high aspect ratio, and consist of both crystalline and amorphous regions.130 The degree of crystallinity and their morphology depend on the cellulosic material used for their production (usually wood, cotton, wheat and rice straw, tunicin, bacteria, and algae), as well as on the preparation conditions and techniques used. Besides being good for strength, reinforcement, and rheology modification, CNCs are also good for the enhancement of optical, electrical, and chemical properties.131 CNC has good biocompatibility and can be stably dispersed into nanoparticles in aqueous media. More importantly, the introduction of CNC can enhance the mechanical strength of hydrogels.132 Cui et al.133 found that the addition of CNC significantly improved the thermal stability and mechanical properties of the hydrogel. Within a certain range, the enhancement effect was proportional to the concentration of CNC. More importantly, through temperature adjustment, the CNC-enhanced hydrogel could be extruded and printed. The printed objects had high resolution and fidelity, and the structure was effectively maintained. Moreover, hydrogels have good biocompatibility and high cell viability. This simple yet effective strategy enables the addition of hydrophilic rigid nanoparticles, such as CNC, to improve the mechanical properties of the soft hydrogel, which makes it capable of meeting the requirements of 3D bioprinting. A liquid bio-resin containing GelMA and polyethylene glycol diacrylate (GPCD) was prepared using T-CNC@CDs (‘CDs’ stands for carbon dots) for digital light processing-based bioprinting. The shear-thinning performance of GPCD bioprinting was further improved by adding T-CNC@CDs, allowing for high-resolution 3D printing and bioprinting of human cells with higher cytocompatibility (survival rate ~95%). The elastic modulus of the printed GPCD hydrogel is ~13±4.2 kPa, making it an ideal material for tissue engineering. Due to the addition of T-CNC@CDs, the prepared hydrogel scaffolds have adjustable structural color properties.
3.3.3. Halloysite nanotubes
Halloysite nanotubes (HNTs) are novel natural one-dimensional particles with a unique tubular microstructure and an aspect ratio of ~20. HNTs have wide applications in catalysis, ceramics, nano-reactors, cosmetics, and polymer nanofillers.134 As reinforcement for polymers used in tissue engineering scaffolds, the tubes have advantages over other nanoparticles, such as hydrophilicity, good dispersion ability, biocompatibility, entrapment of drugs, and low cost.135 Huang et al.136 investigated SA/HNTs composites and reported that HNTs could improve the mechanical properties of the composite hydrogels. Their results also show that the compressive stress of SA/HNTs biomaterials containing 80% HNTs at 80% strain is 2.99 MPa, while the compressive stress of pure SA hydrogel is 0.8 MPa. Zineh et al.137 used Russian olive (RO) powder for bioprinting alginate/HNT/methylcellulose. Mechanical and biological characterizations indicated that the composition containing 20 mg/mL alginate, 20 mg/mL methylcellulose, and 10 mg/mL HNT solution when mixed with 10 mg/mL RO fruit and seed powder, increased chondrocyte viability by 11%. Considering the increase in chondrocyte viability and the enhancement of mechanical properties, this also confirms that the application of HNT in cartilage and osteochondral tissue engineering has considerable prospects.
4. Bioprinting for different kinds of cartilage engineering
4.1. Three-dimensional bioprinting for articular cartilage
Articular cartilage is the cartilage tissue attached to the joint surface, which is a connective tissue composed of ECM of collagen, proteoglycans, and water. In the mature cartilage matrix, about half of the dry weight consists of type II collagen fibers.149,150 The only cell types in articular cartilage are chondrocytes, and depending on the structure and ratio of extracellular tissues to cells, articular cartilage can be divided into four main regions: superficial (10–20%), middle (40–60%), lower (30%), and calcified layers. The superficial layer consists of the thinnest collagen fibers of the highest density, forming oriented lamina splendens that cover the joint. It resists shear, monitors fluid permeability, and contributes to tensile strength. The transition zone contains the highest proteoglycan content, and the collagen orientation varies from tangential to random in the underlying area. Collagen fibers are positioned vertically in the deeper zones and are circled at tidal points, thus separating the deep zone from the calcified zone151,152 (Figure 3A). This arrangement of collagen promotes the fusion of hard and soft tissues at the cartilage–bone interface. In contrast, the calcified zone is composed of collagen X, which is used for mineralization and to maintain structural integrity.7 Due to its unique composition, articular cartilage has excellent mechanical properties, as it transmits loads from the joint to the underlying subchondral bone, absorbing impact forces and promoting smooth, low-friction, and gliding movements of the joint. However, under prolonged mechanical loading, the cartilage layer gradually becomes thinner, and the lack of vascular tissue in cartilage tissue and the low activity of chondrocytes make the cartilage tissue limited in its ability to repair.153 As an emerging technology, 3D bioprinting can mimic the original tissue in terms of structure and function. For the repair of articular cartilage, the main points are to mimic the mechanical properties of cartilage tissue, to be able to maintain long-term viability after the print is implanted in the body, and to stimulate the regeneration of the original tissue in the body.

Figure 3. Histologic characteristics of articular cartilage and 3D printing for the construction of cartilaginous tissues. (A) Schematics of the histological structure of articular cartilage. Reprinted with permission from ref.151 Copyright © 2017, Elsevier Ltd. (B) The composite scaffold of PLA scaffold and hydrogel scaffold provides mechanical and biological properties for cartilage tissue repair similar to those of natural cartilage tissue. Reprinted with permission from ref.156 Copyright © 2020, Elsevier Ltd. (C) Schematic diagram of the structure of the handheld printing device. (D) Cell proliferation viability of structures after printing on days 1 and 15. Reprinted with permission from ref.172 Copyright © 2017, Nature Publishing Group. Abbreviations: HA: Hyaluronic acid; PLA: Polylactic acid; STZ: Superficial tangential zone.
The fabrication of structures with mechanical properties comparable to those of cartilage tissue is one of the goals of 3D bioprinting for cartilage tissue repair. There are several approaches to simulate the mechanical properties of cartilage tissue, such as adding secondary scaffolds,154 creating interpenetrated networks,155 or incorporating solid particles.156 Antich et al.63 deposited a combination of HA and alginate inks in pre-designed PLA scaffolds to assemble cartilage-like tissue scaffolds with mechanical properties similar to those of normal human cartilage tissue for cartilage tissue repair. They mixed chondrocytes with HA/alginate ink and crosslinked them into a gel after injection into the PLA scaffold gap, resulting in a hybrid scaffold. This scaffold was cultured and showed that chondrocytes could remain active and had normal cellular functions63 (Figure 3B). Schipani et al.157 composed a scaffold structure with comparable mechanical properties to cartilage tissue by depositing an interpenetrating network of alginate and GelMA in PCL scaffolds. Their results showed that the mechanical properties of the composite scaffold were higher than those of the scaffold alone, cell cultures showed stable cell growth with collagen secretion, and calcium deposition was observed after longer incubation. Boere et al.158 combined poly(hydroxymethylglycolide-co-e-caprolactone)/poly(e-caprolactone) functionalized with the ability to photocrosslink, and then the hybrid scaffold was photocrosslinked with chondrocyte-loaded GelMA solution to form a composite structure. The results showed that the chondrocytes in the composite structure could survive normally and secrete GAG with type II collagen after 6 weeks of in vitro culture. The addition of microparticles to the hydrogel ink can carry cells for bioprinting while enhancing the strength of the hydrogel,159 and the addition of nHA to bioink is one of the common methods.160 With the addition of nHA, the scaffolds printed by composite inks are conferred a tougher mechanical property than those printed by ink alone. Meanwhile, nHA stimulates the differentiation of BMSCs, accelerating tissue repair and mimicking the mechanical properties of tissues.161
In addition to achieving bionic scaffold mechanical properties, another important factor is to achieve functional scaffolds. Currently, there are two main ways to make printed structures functional: (i) by loading cytokines or drugs in the ink to maintain cellular function and (ii) by guiding cell differentiation. A common strategy is to mix cytokines with hydrogel ink, but this approach is less efficient because of the leakage of drugs or cytokines.162 A more long-lasting approach is to combine cytokines with ink to anchor them in the scaffold structure. Hauptstein et al.163 generated functionalized bioink by modifying HA so that TGF-β1 was covalently linked to HA, and experimentally demonstrated that the modified bioink did not differ significantly from HA ink in printability, while it was significantly more effective at promoting differentiation of MSCs than the scaffold containing TGF-β1 and the scaffold printed with HA, which may be explained by the fact that cells may endocytose TGF-β1 after mixing alone, while TGF-β1 can be slow-released to promote cell differentiation after covalent linkage.163 Similarly, Shi et al.164 covalently crosslinked antioxidants on HA to eliminate ROS in the pathogenesis of osteoarthritis. Also, HA-based hydrogels promote stem cell differentiation to cartilage and ECM deposition.164 By combining cytokines with the substrate hydrogel, it is possible to slow down the action of cytokines in the post-printed structures, allowing them to act long-lastingly on the cellular and extracellular environment.
The other way to build up a functional scaffold is to inoculate cells in the ink and follow the ink to build the intended structure,165 where, for the repair of articular cartilage tissue, the most applied cells are chondrocytes and stem cells. Loaded chondrocytes for printing require a post-printed structure that maintains the activity of the cells and maintains the cartilage phenotype.166 In contrast, loaded BMSCs for printing need to maintain cell activity while guiding cell differentiation toward cartilage and forming cartilage-like tissues. Olate-Moya et al.167 used photocrosslinked alginate as a base, added gelatin and chondroitin sulfate to mimic the ECM of chondrocytes, and then added graphene oxide to provide guidance for cell proliferation and differentiation. Their results showed that MSCs in composite hydrogels survived longer, had higher cell viability, and showed chondrogenic differentiation in the absence of external factors compared to alginate hydrogels alone. Ni et al.168 used a double network structure of silk proteins for bioprinting of loaded BMSCs, and the printed structures could reach normal mechanical strength of the cartilage, and BMSCs can maintain high activity, further proliferate, and differentiate after printing. In addition to BMSCs, other types of stem cells have been used for cartilage tissue repair, such as adipose-derived mesenchymal stem cells (AD-MSCs)169 and articular cartilage-resident chondroprogenitor cells (ACPCs). Levato et al.170 compared the regenerative and constructive abilities of chondrocytes, BMSCs, and ACPCs in GelMA solution and used GelMA as the basis for the construction of ACPCs. Their results showed that collagen and GAG showed a layered distribution in different regions, and ACPCs were less capable of forming calcified cartilage and more suitable for in vitro cartilage tissue construction because of their enhanced lubrication ability compared to BMSCs.
Inevitably, cell activity decreases during cell-laden printing, where shear forces during extrusion or ejection by the nozzle, changes in pH during crosslinking, or UV light exposure can reduce cell viability. Therefore, maintaining high cellular activity during printing is also an issue to be considered for 3D bioprinting. An emerging approach is to encapsulate stem cells (BMSCs) in hydrogel microspheres for 3D bioprinting, which can protect the cells inside and reduce the effect of shear forces on the cells to keep them highly active after printing. Xu et al.171 prepared alginate/gelatin microspheres encapsulated with BMSCs using electrospray and printed the microspheres into PCL scaffolds for cartilage tissue repair. While providing protection, the microsphere hydrogels provided a cartilage–ECM-like environment for stem cells, aiding chondrogenic differentiation of stem cells.171 A more relevant approach for clinical applications is to print out 3D scaffolds in situ for in situ cartilage repair. Duchi et al.172 designed handheld 3D printers that can print out scaffolds in a coaxial fashion. The authors designed a composite bioink using 10 wt% GelMA with 2 wt% HAMA, added AD-MSCs to the core for shell/core bioprinting, and performed in situ photocrosslinking after printing. After cross-linking, the structure yielded a compliant modulus, and the cells still had the ability to proliferate and differentiate after printing, with the potential for in situ cartilage repair172 (Figure 3C and D).
4.2. Three-dimensional bioprinting for osteochondral complex
Osteochondral tissue is the transitional structure connecting articular cartilage to bone tissue, specifically when cartilage tissue reaches the very bottom of the subchondral bone173 (Figure 4A). In osteoarthritic disease, the destruction of cartilage tissue often also invades the underlying osteochondral areas. The overall repair of osteochondral tissue is one of the means of treating osteoarthritis and is also important for cartilage regeneration and the connection of cartilage to the underlying bone.174 For the anisotropic structure of osteochondral bone, 3D bioprinting has the unique advantage that it can print a layered structure of osteochondral tissue according to the design to achieve structural biomimetics. The goal of osteochondral tissue repair is to establish a smooth transition of soft and hard tissue layering and to achieve high activity and normal function when different cells coexist.

Figure 4. Histological characteristics of osteochondral tissues and 3D bioprinting for the construction of osteochondral tissues. (A) The detailed structure of osteochondral tissue. Reprinted with permission from ref.173 Copyright © 2018, Springer. (B) After 6 weeks of osteochondral bidirectional scaffold implantation in nude mice, white hyaline-like tissue appeared in the cartilage region, while vascular-like tissue and mineral deposits appeared in the bone region. Reprinted with permission from ref.43 Copyright © 2020, Elsevier Ltd. (C) Construction of a mimic osteochondral repair scaffold based on the detailed structure of osteochondral tissue (articular cartilage, calcified cartilage, and subchondral bone). Reprinted with permission from ref.178 Copyright © 2020, Nature Publishing Group. (D) Construction of a gradient composite scaffold using PCL and hydroxyapatite microspheres, where the pure PCL layer serves as the cartilage portion, the middle is the transition portion, and at the bottom is the bone formation portion. Reprinted with permission from ref.180 Copyright © 2017, Elsevier Ltd. (E) Schematic diagram of the structure of osteochondral tissue constructed by a technique based on microgel suspension printing. Reprinted with permission from ref.182 Copyright © 2023, Elsevier Ltd. Abbreviations: BMP-2: Bone morphogenetic protein 2; DAH: Diaminohexane; HA: Hyaluronic acid; hTMSCs: Human turbinate mesenchymal stromal cells; PCL: Polycaprolactone; SLS: Selective laser sintering; TGF-β: Transforming growth factor beta.
Critchley et al.175 reported a method to construct osteochondral tissue repair. They used PCL to build a network to enhance mechanical strength, injecting alginate with BMSCs at the bottom of the network gap and alginate containing fat pad-derived stem cells and chondrocytes at the top of the network gap, together forming a bidirectional tissue repair element with mechanical properties comparable to those of human cartilage tissue. After 5 weeks of in vitro culture, chondrocytes in the cartilage fraction had higher cell viability compared to the unidirectional hydrogel. The repair element was transplanted subcutaneously into nude mice, and after 6 weeks a clear interface between the cartilage and bone fractions could be seen, with abundant vascularization in the bone tissue fraction and no vascularization in the cartilage fraction. In contrast to unidirectional hydrogels, endochondral osteogenesis was negligible in bidirectional elements.175 Shim et al.43 used multiple inks deposited alternately to form an osteochondral repair scaffold. They used PCL as a base scaffold, building PCL layer by layer and extruding bioinks layer by layer, extruding pepsin-treated collagen containing bone morphogenetic protein 2 (BMP-2) and human turbinate mesenchymal stromal cells (hTMSCs) as the osteogenic portion at the bottom and mono-functionalized cucurbit uril-conjugated HA, which contains hTMSCs and TGF-β as the chondrogenic fraction, to form an osteochondral repair scaffold. The modified HA hydrogels showed significant cartilage tissue regeneration after 8 weeks of in vitro culture without the toxic effects of conventional HA hydrogels, while in the osteogenic fraction, new bone tissue was deposited in large quantities around the PCL scaffold, showing good osteochondral repair potential43 (Figure 4B). HA is one of the components of the cartilage ECM and has some advantages over other inks in cartilage repair, while the use of chondrocyte dECM as a bioink allows the introduction of multiple components into chondrocyte culture that more closely resembles the growth of native cartilage tissue.176 The mechanical strength of the overall structure can be increased by a dual scaffold approach, such as the use of PCL scaffolds. However, it also increases the complexity of the processing, and the adhesion between the mechanical scaffold and the bioink may affect the stability of the overall structure. A more biomimetic approach relies on bioink to achieve the desired mechanical properties of the scaffold. Chen et al.177 developed novel hydrogels using SA and gellan gum hybridized with inorganic thixotropic magnesium phosphate-based gels in a pre-crosslinking of Mg2+. By adjusting the ratio of the components, it is possible to achieve a modulation for the mechanical properties of the printed scaffold to achieve the desired strength, and osteoblasts can proliferate and synthesize ECM in the hydrogel ink. Importantly, when BMSCs are cultured in this hydrogel, a differentiation of BMSCs toward both osteogenic and chondrogenic directions can be observed, and although the exact mechanism is not known, they show potential for osteochondral repair.177
In addition to viewing the osteochondral structure as a two-part structure, more elaborate bioengineering can build osteochondral repair scaffolds through multilayered structures. One study was conducted by designing chondrocyte-loaded methylcellulose alginate as a surface chondrogenic structure, chondrocyte-loaded methylcellulose alginate, and calcium phosphate cement as a calcified cartilage structure, and calcium phosphate cement as the lowermost layer. After deposition as a composite structure, chondrocytes can maintain a high viability within the scaffold178 (Figure 4C). A more precise way is to establish a gradient structure179 to achieve a smooth transition between the interfaces. Du et al.123 used hydroxyapatite with PCL microspheres to establish a hydroxyapatite gradient scaffold under the selective laser sintering technique. The particle size of HA was 80–100 nm, and the content of HA in the scaffold ranged from 30 to 0 wt% from the bottom to the top layer, forming a vertically continuous HA gradient in the pure PCL microsphere layer as a chondrogenic layer, in the middle low HA content is the transition layer, and in the bottom is the subchondral bone formation layer. A large number of pores were formed inside the stent to facilitate cell growth into it. After inoculation of BMSCs, the cell proliferation rate was significantly higher compared to the normal PCL scaffold and showed significant osteogenic differentiation, while 12 weeks after implantation of the scaffold into the rabbit osteochondral defect model, new cartilage tissue and bone tissue growth could be observed, and the newly formed cartilage tissue was similar in thickness to the surrounding native tissue, and the interface between cartilage and subchondral bone was well integrated, and no bone to bone overgrowth was observed180 (Figure 4D). Hinton et al.181 invented a printing technique called FRESH, which simply means that the ink is deposited into a support bath composed of microspherical hydrogels, allowing for free printing and more diverse modulation. Based on this, Jalandhra et al.182 added adipose-derived stem cells (ADSCs) in a support bath composed of gelatin microspheres and then printed in the support bath with α-tricalcium phosphate as ink, and bioink was deposited onto the surface of the microspheres, causing ADSCs close to the ink trajectory to differentiate toward osteogenesis and cells far from the ink trajectory to differentiate toward chondrogenesis, achieving the establishment of an osteochondral interface, which is expected to be a new method for osteochondral repair (Figure 4E). In future studies, gradient repair scaffolds may be the most favorable means of osteochondral repair.
4.3. Three-dimensional bioprinting for meniscus
The meniscus, similar to other articular cartilages, is highly anisotropic and a complex tissue along its depth with different cellular composition, biochemical composition, and macromolecular orientation.183 However, cartilage is an avascular tissue with poor regenerative capacity, especially on the medial side of the meniscus, and injury is characterized by low healing potential. The anatomy of the knee (including the meniscus) is shown in Figure 5A. The meniscus, once damaged, has a greater likelihood of eventually developing osteoarthritis, particularly when treated with meniscectomy modalities.184,185

Figure 5. Anatomical composition of the human knee including menisci (A) and human intervertebral disc (B). Reprinted from ref.186
In recent years, surgical techniques, allogeneic transplantation, autologous chondrocyte implantation, bone marrow stimulation, and mosaicplasty have been used in attempts to repair the meniscus, but all have their own limitations.187–189 There are increasing studies on the application of 3D bioprinting for meniscal repair. To be as similar as possible to the native meniscus, the mechanical properties, mechanical stability, tribological properties, biocompatibility, porosity, cell colonization requirements, and adequate degradation profile need to be maintained.190 Insufficient resolution, structural inhomogeneity, and anisotropy of the meniscus are issues to be addressed with 3D bioprinting. Bahcecioglu et al.191 designed a PCL/hydrogel structure that can mimic the structural organization, biochemistry, and anatomical structure of the meniscus. Cell-loaded GelMA was impregnated around an anatomical scaffold with a PCL loop strand, and cell-loaded GelMA-Ag was internally impregnated. GelMA and GelMA-Ag hydrogels increased the yield of type I collagen and type II collagen proteins after 6 weeks of culture. They believe that the Young’s modulus, porosity, and ultrastructure of the scaffolds may affect meniscus regeneration. 3D bioprinting can mimic the structural inhomogeneity and anisotropy of fabricated menisci.
However, there are still several problems with 3D bioprinting for meniscus repair.190 The first is the technical aspect, in which material viscosity, shear force, crosslinking method, and maintenance of 3D shape all affect cell viability, material resolution, and porosity. The second issue is the scaffold. No biomaterial that is mechanically strong, biocompatible, and can promote cell viability has yet been identified. In addition, one material cannot be used simultaneously to support a specific cell phenotype and to have the desired printing properties. The third problem is the cells. Since meniscal fibrochondrocytes (MFCs) have sufficient fibrocartilaginous differentiation potential and can form collagen fibers similar to those of the native meniscus. Furthermore, MFCs have less tendency to form bone precursors leading to calcification than MSCs. However, MFCs have been isolated in lower numbers from surgical specimens.
4.4. Three-dimensional bioprinting for intervertebral disc
The intervertebral disc (IVD) mainly includes the nucleus pulposus, AF, and cartilage endplate. The IVD is mainly composed of the nucleus pulposus, AF, and cartilaginous endplates (Figure 5B). Three components have their own characteristics. The main components of the nucleus pulposus are proteoglycans, water, and type II collagen. The AF is characterized by a high density of type I collagen and less water and proteoglycans. The cartilaginous endplates were hyaline avascular cartilaginous tissue.
Discectomy, disc replacement, and spinal fusion are currently commonly used in the clinic to treat disc pathologies. However, none of these treatment modalities can restore tissue function to the disc, leading to changes in spine biomechanics.192,193 As the functions and structures of each zone of the disc are different, 3D bioprinting, which enables precise control over each zone, has unique advantages. Loss of hydration is one of the theoretical bases leading to degenerative disc degeneration. 3D bioprinting has been widely used to create highly hydrated nucleus pulposus in recent years.194 But the greatest technical difficulty remains in the disc’s structural and functional complexity. One point to be noted for the application of 3D bioprinting to repair IVDs is that the high mechanical loads that the discs bear can negatively affect the function of these hydrogels compared to other cartilages. Thus, there is a need to develop bioink at high resolution that reconstitutes complex tissue networks, supports cell function, and handles large loads in the spine.195 More studies are needed in the future to design biomimetic discs with optimal structural, biomechanical, and biological properties to achieve the repair of disc tissue. Since the spine would bear high-strength pressure loads, it is more demanding for the mechanical strength of 3D bioprinting to repair disc tissue, and high mechanical loads can negatively affect the function of these hydrogels. Therefore, the main challenge is to develop high-resolution extrusion-type bioink that reconstitutes complex tissue networks that support cell function while being required to bear the large load in the spine.195 To address the above difficulties, 3D bioprinting using synthetic bioink has been commonly performed in recent years. Combining mechanically tough polymers with printable polymers to improve, resulting in double network hydrogels that can be rapidly and efficiently printed while promoting spinal integration with sufficient mechanical strength.196 Moxon et al.197 3D-printed biphasic hydrogel structures composed of gellan gum and type I collagen, simulating nucleus pulposus and AF regions, respectively. Not only did it summarize the microstructural features of these regions, but it also promoted the incorporation of nucleus pulposus and AF cell lines. In addition, they found that the same effect can be triggered when IVD cells are replaced by human MSCs, demonstrating the potential of using suspended layer additive manufacture bioprinting to control stem cell phenotype and morphology by regulating the structure of the extracellular environment. IVD-based analogs are not only expected to be used to study the mechanism of IVD-like tissue formation but also to expand their application scope from IVD biology to a wider range of tissue engineering and regenerative medicine fields. Sun et al.198 3D-printed a material consisting of biomaterials, cells, connective tissue growth factor, and TGF-β3 loaded onto polydopamine nanoparticles, mixed with BMSCs for regeneration and simulation of the structure and function of the nucleus pulposus and AF. In vitro experiments have shown that printed BSMCs can maintain high activity and differentiate into myeloid cells and fibrous ring-like cells. The prepared scaffold was implanted subcutaneously into the back of nude mice, and the IVD was reconstructed in a band shape, displaying the specific matrix of the corresponding histological and immunological phenotype.
4.5. 3D bioprinting for other cartilage
Auricular cartilage provides shape, structural support, and shock absorption.199 Loss of auricular cartilage leads to microtia. Autologous costal cartilage is commonly used in patients with microtia to create an auricular framework. However, this treatment modality is usually associated with high requirements for surgeon skills, donor site morbidity, pain intensity, and the risk of causing pneumothorax after surgery.200 In addition, silicone frameworks used as surgical material suffer from graft rejection, frameshift, time-consuming production, and other disadvantages.201 The advent of 3D bioprinting has been a boon in solving these problems. 3D bioprinting of ear tissue allows for the replication of auricular anatomy, mimicry or embedding of elements of the ECM, and adhesion and lineage commitment of cells before and after implantation in vivo.201 However, as the external auricle primarily relies on cartilage for structural support, the adequacy of biodegradable materials’ mechanical strength remains a subject of debate.202 3D bioprinting technology, compared with traditional autologous rib grafting surgery methods, can reduce many surgical risks, alleviate pain in patients, eliminate the need for surgeons to remove the ribs and then perform manual trimming based on the contralateral ear (surgical outcomes are influenced by the operating surgeon) and other advantages. However, there are still some obstacles in the application of 3D bioprinting technology to repair ear cartilage tissue for pre-clinical use.203 First, the scalability of bioprinting materials needs to be addressed urgently. Second, currently available 3D bioprinting technologies are still too complex for large-scale production. In addition, the cellularized scaffolds suffer from a shrinkage phenomenon due to the high degree of interaction between cells within the remodeled hydrogels, causing deformation of the implanted structures. In addition, adequate reepithelialization of the construct after implantation remains a challenge, along with the high costs associated with cell collection and expansion prior to construction manufacturing under good manufacturing practice conditions.204,205
In addition, nasal septal cartilage is a promising field for cartilage tissue engineering. Septal cartilage is a key supporting structure in the framework of the human nasal cavity. Nasal scaffold deformity and nasal obstruction due to collapse or absence of septal cartilage may be caused by trauma, tumor, aging, or previous surgery. Current typical options for nasal stent reconstruction include autologous, allogeneic, or synthetic sources.206 Nasal septal cartilage tissue engineering has the potential to provide surgical options for patients with complex reconstruction needs, mitigate other risks caused by existing tissue sources, and reduce the risk of immune exclusion, disease transmission, and resorption from allogeneic sources.207 At the same time, similar to ear cartilage tissue engineering, it reduces the pain and risk of autologous bone grafting, such as costal cartilage, for patients.208 Shokri et al.209 used 3D-printed elastomin–gelatin–HA scaffolds and chondrocytes for in vivo regeneration of nasal septal cartilage defects and successfully reduced the average residual defect area. Lan et al.210,211 conducted a series of studies. In the first step, they successfully generated engineered nasal septal cartilage by employing a free-form reversible embedding (FRESH) bioprinting method with type I collagen hydrogel, in which in vitro biochemical results were highly similar to those of native tissue.210 The clinical application and potential to form patient-specific surgical-ready shapes, mechanical characterization, and in vivo stability of the engineered nasal cartilage substitute were further validated.211 With the ability to 3D-bioprint patient-specific inferior lateral cartilage, Lan et al.210 subsequently investigated the effect of chondrogenic cultures on biochemical and mechanical properties of bioprinted constructs of human nasal chondrocytes in vitro and in vivo using nude mice.
5. From laboratory to clinical practice
The regeneration of cartilage and osteochondral tissue is known to be a time-consuming process. Unfortunately, the ever-increasing incidence of injuries or diseases that cause cartilage and osteochondral damage further adds to the disease burden every year.212 Therefore, new effective strategies are needed to treat and replace cartilage and osteochondral tissue. To this end, 3D bioprinting provides a promising platform for the rapid production of cartilage and osteochondral tissue aimed at replacing diseased cartilage and osteochondral tissue. Over the past few years, 3D bioprinting has undergone an evolution from the proof-of-concept printing model to another that enables the fabrication of complex multicomponent tissue-like constructs similar to their in vivo counterparts. Complete translation of tissue bioprinting presents huge challenges in a clinical context, in particular, achieving 3D-bioprinted tissue fully embodying the reconstruction of damaged tissues, such as cartilage or osteochondral tissues, would take a long time. However, to date, only a few studies have successfully evaluated the performance of bioprinting constructs in an in vivo setting. More investigations are warranted to attempt to construct implantation in real-world environments to demonstrate the possible translation from research to the clinic. Thus, given the long-term process involved in the full clinical translation of bioprinted constructs, robust and systematic evaluations are needed to demonstrate the in vivo applicability of bioprinted constructs.3 In addition, 3D-bioprinted scaffolds may elicit immune responses in vivo, a facet of this technology that requires in-depth exploration in specific cases.
The first aspect that we should consider in the translation of bioprinting from laboratory to clinic is the compatibility of biomaterials with cells. Biomaterials should not only provide physical support for cells but also have good biocompatibility to ensure cell survival, proliferation, and differentiation. How to optimize the formulation of biomaterials to better match the needs of cell growth is one of the key issues in clinical translation. In addition, cell source and quality are critical factors. Although immune rejection cases are minimal in the usage of autologous cells, the amount of obtained cells is limited, and there is a risk of donor site damage. Although allogeneic or stem cell-derived cells can address the quantity issues, they may elevate the risks of immune reactions. Thus, the last few years have been devoted to the development of more biocompatible bioinks to allow replication of organ-specific ECM while maintaining high cell viability and activity as well as induction of organ-specific ECM. However, the organ-specific ECM affords a rather “synthetic” environment, which may induce organ-like behavior of cells but hardly mimics the full composition of the native ECM in human tissues. In recent years, the dECM—typically derived from animals’ organs—has been discovered as an excellent candidate bioink, by virtue of the reduced severe immune rejection and provision of a specific environment for tissue repair or tissue regeneration.213 Furthermore, Faramarzi et al.214 developed bioinks that include patient’s autologous material obtained from platelet-rich plasma for patient realization—their approach shows that patient-specific tissues can be obtained by bioprinting and that the use of autologous materials is a key factor in ensuring tissue performance and transplantability, especially in the clinic.
Another challenge facing the clinical translation of bioprinting is striking a balance between printing accuracy and structural complexity. Achieving accurate 3D-printed structures is essential to simulate the complex structures of natural cartilage and osteochondral tissues. However, challenges remain in achieving micron-scale printing accuracy at the current state, posing difficulty in fully reproducing the fine structure of natural tissues, such as the layered structure of cartilage and the complex connection of osteochondral interfaces. Parameter fluctuations during the printing process, such as temperature and pressure changes, also affect the printing accuracy. Improving the accuracy and stability of printing, as well as being able to print tissue constructs with complex internal structures, are prerequisites for effective clinical application.
In addition, the speed of printing is also a noteworthy factor in order to achieve translation from laboratory to clinic.3 The common drawback of current bioprinting systems is the fabrication of complex biomimetic tissues based on low printing speed. This is a significant limitation for the clinical application of bioprinting, as bioprinting larger tissues may outspend the time for on-demand tissue creation. Several studies have focused on reducing the time required by using a single nozzle to store multiple materials in extrusion-based bioprinting.215 However, stereolithography has so far not been able to achieve the versatility of extrusion-based bioprinting, and only a few studies have successfully integrated multiple materials into stereolithography-based systems.216 Increasing the speed of bioprinting is an important step toward the clinical translation of bioprinting and the on-demand manufacturing of biologically relevant tissue structures.
Finally, although many studies have been conducted to promote the translation of 3D bioprinting from the laboratory to the clinic in the past few years, some studies have only remained at the cellular level. Demonstrating scaffold function in real-world environments is a key step to achieving clinical translation. In vivo experiments should be an important part of all bioprinting studies that focus on the fabrication of biomimetic tissues suitable for clinical applications. In addition, the long-term efficacy and safety of 3D-printed cartilage and osteochondral regeneration products need to be fully evaluated before clinical application. The long-term efficacy is a multifaceted parameter encompassing the durability of tissue repair, the recovery of mechanical properties, and whether it can effectively relieve the symptoms of patients. In terms of safety, in addition to the risks related to biological materials and cells, potential contaminants or impurities introduced during the printing process should also be considered. At present, how to establish a perfect long-term efficacy and safety evaluation system is an urgent problem to be solved in the process of clinical translation. However, there are still some obstacles in applying 3D bioprinting technology to repair nasal septal cartilage tissue for pre-clinical applications.206 The first is to tackle the need for an adequate source of autologous cells. Typically, fewer cells would be needed from the harvested cartilage at the time of surgery if a higher cell density can be achieved within a shorter culture period. Using appropriate media and bioreactors can help achieve this. In addition, while chondroprogenitor cells can provide a more abundant source of cells, it is also necessary to control their growth. The second obstacle is to establish effective scaffolds and bioinks. Ideally, the scaffold would appropriately interact with the selected cell type in terms of cell adhesion, proliferation, and redifferentiation. In addition, the scaffold will provide appropriate mechanical properties for reconstruction. Hybrid stents appear to be particularly promising.
6. Conclusion and perspectives
3D bioprinting is a promising technology for cartilage and osteochondral regeneration. Cartilage and osteochondral defects are common injuries that can lead to severe pain, impaired joint function, and decreased quality of life. Traditional treatment methods for cartilage and osteochondral injuries have limitations, and many patients require joint replacement surgery. By allowing for the creation of patient-specific, biocompatible constructs that can regenerate damaged tissue, 3D bioprinting offers a potential solution to this problem, essentially leading to reduced pain, improved joint function, and a higher quality of life for patients suffering from cartilage and osteochondral injuries.
In conclusion, 3D bioprinting has the potential to revolutionize the field of cartilage and osteochondral regeneration. The technology allows for the precise placement of cells and biomaterials in a 3D environment, creating constructs that mimic the native tissue structure and function. Although the technology is still in its infancy, numerous studies have demonstrated its effectiveness in pre-clinical models, and clinical trials are underway. Ultimately, 3D bioprinting has the potential to become a mainstream treatment option for these conditions, offering a personalized, effective, and long-lasting solution to patients worldwide.
Looking ahead, the development of 3D bioprinting technology for cartilage and osteochondral regeneration is likely to progress at a rapid pace. We anticipate that advances in biomaterials, cell sourcing, and printing techniques could overcome many of the existing challenges. Nevertheless, challenges, such as the scalability of the technology, the need for suitable biomaterials, and regulatory hurdles, remain to be surmounted.
1.Vacanti JP, Langer R. Tissue engineering: the design and fabrication of living replacement devices for surgical reconstruction and transplantation. Lancet. 1999; 354(Suppl 1):SI32-S134.
doi: 10.1016/s0140-6736(99)90247-7
2.Zhang YS, Yue K, Aleman J, et al. 3D bioprinting for tissue and organ fabrication. Ann Biomed Eng. 2017;45(1):148-163.
doi: 10.1007/s10439-016-1612-8
3.Heinrich MA, Liu W, Jimenez A, et al. 3D Bioprinting: from benches to translational applications. Small (Weinheim an der Bergstrasse, Germany). 2019;15(23):e1805510.
4.Ravanbakhsh H, Bao G, Luo Z, Mongeau LG, Zhang YS. Composite inks for extrusion printing of biological and biomedical constructs. ACS Biomater Sci Eng. 2020;7(9):4009-4026.
doi: 10.1021/acsbiomaterials.0c01158
5.Montesdeoca CYC, Stocco TD, Marciano FR, Webster TJ, Lobo AO. 3D bioprinting of smart oxygen-releasing cartilage scaffolds. J Funct Biomater. 2022;13(4):252.
doi: 10.3390/jfb13040252
6.Mei Q, Rao J, Bei HP, Liu Y, Zhao X. 3D bioprinting photo-crosslinkable hydrogels for bone and cartilage repair. Int J Bioprint. 2021;7(3):367.
7.Zhang L, Hu J, Athanasiou KA. The role of tissue engineering in articular cartilage repair and regeneration. Crit Rev Biomed Eng. 2009;37(1-2):1-57.
doi: 10.1615/critrevbiomedeng.v37.i1-2.10
8.Luo Z, Mu X, Zhang YS. Biomaterials for bioprinting. Bioprinting. Academic Press; 2022:51-86.
doi: 10.1016/B978-0-323-85430-6.00001-7
9.Luo Z-Y, Wang H-Y, Wang D, Zhou K, Pei F-X, Zhou Z-K. Oral vs intravenous vs topical tranexamic acid in primary hip arthroplasty: a prospective, randomized, double-blind, controlled study. J Arthroplasty. 2018;33(3):786-793.
doi: 10.1016/j.arth.2017.09.062
10.Luo Z-Y, Li L-L, Wang D, Wang H-Y, Pei F-X, Zhou Z-K. Preoperative sleep quality affects postoperative pain and function after total joint arthroplasty: a prospective cohort study. J Orthop Surg Res. 2019;14(1):1-10.
doi: 10.1186/s13018-019-1446-9
11.Jain P, Kathuria H, Dubey N. Advances in 3D bioprinting of tissues/organs for regenerative medicine and in-vitro models. Biomaterials. 2022;287:121639.
doi: 10.1016/j.biomaterials.2022.121639
12.Li X, Liu B, Pei B, et al. Inkjet Bioprinting of Biomaterials. Chem Rev. 2020;120(19):10793-10833.
doi: 10.1021/acs.chemrev.0c00008
13.Mandrycky C, Wang Z, Kim K, Kim DH. 3D bioprinting for engineering complex tissues. Biotechnol Adv. 2016;34(4):422-434.
doi: 10.1016/j.biotechadv.2015.12.011
14.Gudapati H, Dey M, Ozbolat I. A comprehensive review on droplet-based bioprinting: past, present and future. Biomaterials. 2016;102:20-42.
doi: 10.1016/j.biomaterials.2016.06.012
15.Zub K, Hoeppener S, Schubert US. Inkjet printing and 3D printing strategies for biosensing, analytical, and diagnostic applications. Adv Mater. 2022;34(31):e2105015.
16.Kim YK, Park JA, Yoon WH, Kim J, Jung S. Drop-on-demand inkjet-based cell printing with 30-μm nozzle diameter for cell-level accuracy. Biomicrofluidics. 2016;10(6):064110.
doi: 10.1063/1.4968845
17.Bishop ES, Mostafa S, Pakvasa M, et al. 3D bioprinting technologies in tissue engineering and regenerative medicine: current and future trends. Genes Dis. 2017;4(4):185-195.
doi: 10.1016/j.gendis.2017.10.002
18.Hendriks J, Willem Visser C, Henke S, et al. Optimizing cell viability in droplet-based cell deposition. Sci Rep. 2015;5:11304.
doi: 10.1038/srep11304
19.Knowlton S, Onal S, Yu CH, Zhao JJ, Tasoglu S. Bioprinting for cancer research. Trends Biotechnol. 2015;33(9):504-513.
doi: 10.1016/j.tibtech.2015.06.007
20.Prasad LK, Smyth H. 3D printing technologies for drug delivery: a review. Drug Dev Ind Pharm. 2016;42(7):1019-1031.
doi: 10.3109/03639045.2015.1120743
21.Huang J, Xiong J, Wang D, et al. 3D bioprinting of hydrogels for cartilage tissue engineering. Gels. 2021;7(3):144.
doi: 10.3390/gels7030144
22.Gu Z, Fu J, Lin H, He Y. Development of 3D bioprinting: from printing methods to biomedical applications. Asian J Pharm Sci. 2020;15(5):529-557.
doi: 10.1016/j.ajps.2019.11.003
23.Tang G, Luo Z, Lian L, et al. Liquid-embedded (bio) printing of alginate-free, standalone, ultrafine, and ultrathinwalled cannular structures. Proc Natl Acad Sci U S A. 2023;120(7):e2206762120.
24.Rossi A, Pescara T, Gambelli AM, et al. Biomaterials for extrusion-based bioprinting and biomedical applications. Front Bioeng Biotechnol. 2024;12:1393641.
doi: 10.3389/fbioe.2024.1393641
25.Nair K, Gandhi M, Khalil S, et al. Characterization of cell viability during bioprinting processes. Biotechnol J. 2009;4(8):1168-1177.
26.Ravanbakhsh H, Luo Z, Zhang X, et al. Freeform cell-laden cryobioprinting for shelf-ready tissue fabrication and storage. Matter. 2021;5(2):573-593.
doi: 10.1016/j.matt.2021.11.020
27.Yi S, Liu Q, Luo Z, et al. Micropore-forming gelatin methacryloyl (GelMA) bioink toolbox 2.0: designable tunability and adaptability for 3D bioprinting applications. Small. 2022;18(25):e2106357.
28.Wang M, Li W, Hao J, et al. Molecularly cleavable bioinks facilitate high-performance digital light processing-based bioprinting of functional volumetric soft tissues. Nat Commun. 2022;13(1):3317.
doi: 10.1038/s41467-022-31002-2
29.Raman R, Bhaduri B, Mir M, et al. High-resolution projection microstereolithography for patterning of neovasculature. Adv Healthc Mater. 2016;5(5):610-619.
30.Daly AC, Freeman FE, Gonzalez-Fernandez T, Critchley SE, Nulty J, Kelly DJ. 3D bioprinting for cartilage and osteochondral tissue engineering. Adv Healthc Mater. 2017;6(22).
31.Donderwinkel I, van Hest JCM, Cameron NR. Bio-inks for 3D bioprinting: recent advances and future prospects. Review. Polym Chem. 2017;8(31):4451-4471.
doi: 10.1039/c7py00826k
32.Debnath S, Agrawal A, Jain N, Chatterjee K, Player DJ. Collagen as a bio-ink for 3D printing: a critical review. J Mater Chem B. 2025;13(6):1890-1919.
doi: 10.1039/d4tb01060d
33.Rezvani Ghomi E, Nourbakhsh N, Akbari Kenari M, Zare M, Ramakrishna S. Collagen-based biomaterials for biomedical applications. J Biomed Mater Res Part B, Appl Biomater. 2021;109(12):1986-1999.
doi: 10.1002/jbm.b.34881
34.Li M, Sun D, Zhang J, Wang Y, Wei Q, Wang Y. Application and development of 3D bioprinting in cartilage tissue engineering. Review. Biomater Sci. 2022;10(19):5430-5458.
doi: 10.1039/d2bm00709f
35.Hospodiuk M, Dey M, Sosnoski D, Ozbolat IT. The bioink: a comprehensive review on bioprintable materials. Biotechnol Adv. 2017;35(2):217-239.
doi: 10.1016/j.biotechadv.2016.12.006
36.Buma P, Pieper JS, van Tienen T, et al. Cross-linked type I and type II collagenous matrices for the repair of full-thickness articular cartilage defects—a study in rabbits. Article. Biomaterials. 2003;24(19):3255-3263.
doi: 10.1016/s0142-9612(03)00143-1
37.Bosnakovski D, Mizuno M, Kim G, Takagi S, Okumura M, Fujinaga T. Chondrogenic differentiation of bovine bone marrow mesenchymal stem cells (MSCs) in different hydrogels: influence of collagen type II extracellular matrix on MSC chondrogenesis. Article. Biotechnol Bioeng. 2006;93(6):1152-1163.
doi: 10.1002/bit.20828
38.Lee JM, Suen SKQ, Ng WL, Ma WC, Yeong WY. Bioprinting of collagen: considerations, potentials, and applications. Review. Macromol Biosci. 2021;21(1):2000280.
39.Diamantides N, Wang L, Pruiksma T, et al. Correlating rheological properties and printability of collagen bioinks: the effects of riboflavin photocrosslinking and pH. Article. Biofabrication. 2017;9(3):034102.
40.Beketov EE, Isaeva EV, Yakovleva ND, et al. Bioprinting of cartilage with bioink based on high-concentration collagen and chondrocytes. Article. Int J Mol Sci. 2021;22(21):11351.
41.Jiang W, Li L, Zhang D, et al. Incorporation of aligned PCL-PEG nanofibers into porous chitosan scaffolds improved the orientation of collagen fibers in regenerated periodontium. Acta Biomater. 2015;25:240-252.
doi: 10.1016/j.actbio.2015.07.023
42.Rhee S, Puetzer JL, Mason BN, Reinhart-King CA, Bonassar LJ. 3D bioprinting of spatially heterogeneous collagen constructs for cartilage tissue engineering. ACS Biomater Sci Eng. 2016;2(10):1800-1805.
doi: 10.1021/acsbiomaterials.6b00288
43.Shim JH, Jang KM, Hahn SK, et al. Three-dimensional bioprinting of multilayered constructs containing human mesenchymal stromal cells for osteochondral tissue regeneration in the rabbit knee joint. Biofabrication. 2016;8(1):014102.
doi: 10.1088/1758-5090/8/1/014102
44.Asim S, Tabish TA, Liaqat U, Ozbolat IT, Rizwan M. Advances in gelatin bioinks to optimize bioprinted cell functions. Review. Adv Healthc Mater. 2023;12(17).
45.Wang X, Ao Q, Tian X, et al. Gelatin-based hydrogels for organ 3D bioprinting. Review. Polymers. 2017;9(9):401.
doi: 10.3390/polym9090401
46.Sun M, Sun X, Wang Z, Guo S, Yu G, Yang H. Synthesis and properties of gelatin methacryloyl (GelMA) hydrogels and their recent applications in load-bearing tissue. Review. Polymers. 2018;10(11):1290.
47.Sathish PB, Gayathri S, Priyanka J, et al. Tricomposite gelatin-carboxymethylcellulose-alginate bioink for direct and indirect 3D printing of human knee meniscal scaffold. Article. Int J Biol Macromol. 2022;195:179-189.
doi: 10.1016/j.ijbiomac.2021.11.184
48.Re F, Sartore L, Moulisova V, et al. 3D gelatin-chitosan hybrid hydrogels combined with human platelet lysate highly support human mesenchymal stem cell proliferation and osteogenic differentiation. Article. J Tissue Eng. 2019;10:2041731419845852.
49.Wang D, Maharjan S, Kuang X, et al. Microfluidic bioprinting of tough hydrogel-based vascular conduits for functional blood vessels. Sci Adv. 2022;8(43):eabq6900.
50.He H, Li D, Lin Z, et al. Temperature-programmable and enzymatically solidifiable gelatin-based bioinks enable facile extrusion bioprinting. Article. Biofabrication. 2020;12(4):045003.
51.Li J, Zhang Y, Zhou X, et al. Enzymatically functionalized RGD-gelatin scaffolds that recruit host mesenchymal stem cells in vivo and promote bone regeneration. J Colloid Interface Sci. 2022;612:377-391.
doi: 10.1016/j.jcis.2021.12.091
52.Souza A, Kevin M, Rodriguez BJ, Reynaud EG. The use of fluid-phase 3D printing to pattern alginate-gelatin hydrogel properties to guide cell growth and behaviour in vitro. Biomed Mater (Bristol, England). 2024;19(4).
53.Shiwarski DJ, Hudson AR, Tashman JW, Feinberg AW. Emergence of FRESH 3D printing as a platform for advanced tissue biofabrication. APL Bioeng. 2021;5(1):010904.
doi: 10.1063/5.0032777
54.Kupfer ME, Lin WH, Ravikumar V, et al. In situ expansion, differentiation, and electromechanical coupling of human cardiac muscle in a 3D bioprinted, chambered organoid. Circ Res. 2020;127(2):207-224.
doi: 10.1161/circresaha.119.316155
55.Vepari C, Kaplan DL. Silk as a biomaterial. Prog Polym Sci. 2007;32(8-9):991-1007.
doi: 10.1016/j.progpolymsci.2007.05.013
56.Singh YP, Bandyopadhyay A, Mandal BB. 3D bioprinting using cross-linker-free silk-gelatin bioink for cartilage tissue engineering. Article. ACS Appl Mater Interfaces. 2019;11(37):33684-33696.
57.Schacht K, Juengst T, Schweinlin M, Ewald A, Groll J, Scheibel T. Biofabrication of cell-loaded 3D spider silk constructs. Article. Angew Chem Int Ed. 2015;54(9):2816-2820.
58.Burdick JA, Prestwich GD. Hyaluronic acid hydrogels for biomedical applications. Article. Adv Mater. 2011;23(12):H41-H56.
59.Pescosolido L, Schuurman W, Malda J, et al. Hyaluronic acid and dextran-based semi-IPN hydrogels as biomaterials for bioprinting. Article. Biomacromolecules. 2011;12(5):1831-1838.
doi: 10.1021/bm200178w
60.Hauptstein J, Boeck T, Bartolf-Kopp M, et al. Hyaluronic acid-based bioink composition enabling 3d bioprinting and improving quality of deposited cartilaginous extracellular matrix. Article. Adv Healthc Mater. 2020;9(15):2000737.
61.Gong J, Schuurmans CCL, van Genderen AM, et al. Complexation-induced resolution enhancement of 3D-printed hydrogel constructs. Article. Nat Commun. 2020;11(1):1267.
doi: 10.1038/s41467-020-14997-4
62.Antich C, de Vicente J, Jimenez G, et al. Bio-inspired hydrogel composed of hyaluronic acid and alginate as a potential bioink for 3D bioprinting of articular cartilage engineering constructs. Article. Acta Biomater. 2020;106:114-123.
doi: 10.1016/j.actbio.2020.01.046
63.Lee KY, Mooney DJ. Alginate: properties and biomedical applications. Prog Polym Sci. 2012;37(1):106-126.
doi: 10.1016/j.progpolymsci.2011.06.003
64.Jia J, Richards DJ, Pollard S, et al. Engineering alginate as bioink for bioprinting. Research support, N.I.H., extramural; research support, U.S. Gov’t, Non-P.H.S. Acta Biomater. 2014;10(10):4323-4331.
doi: 10.1016/j.actbio.2014.06.034
65.Yang X, Lu Z, Wu H, Li W, Zheng L, Zhao J. Collagen-alginate as bioink for three-dimensional (3D) cell printing based cartilage tissue engineering. Article. Mater Sci Eng C-Mater Biol Appl. 2018;83:195-201.
doi: 10.1016/j.msec.2017.09.002
66.He Y, Derakhshanfar S, Zhong W, et al. Characterization and application of carboxymethyl chitosan-based bioink in cartilage tissue engineering. Article. J Nanomater. 2020;2020(1):2057097.
doi: 10.1155/2020/2057097
67.Lu JX, Prudhommeaux F, Meunier A, Sedel L, Guillemin G. Effects of chitosan on rat knee cartilages. Article. Biomaterials. 1999;20(20):1937-1944.
doi: 10.1016/s0142-9612(99)00097-6
68.Huang H, Zhang X, Hu X, et al. Directing chondrogenic differentiation of mesenchymal stem cells with a solid-supported chitosan thermogel for cartilage tissue engineering. Article. Biomed Mater. 2014;9(3):035008.
doi: 10.1088/1748-6041/9/3/035008
69.Keane TJ, Swinehart IT, Badylak SF. Methods of tissue decellularization used for preparation of biologic scaffolds and in vivo relevance. Review. Methods. 2015;84:25-34.
doi: 10.1016/j.ymeth.2015.03.005
70.Sellaro TL, Ranade A, Faulk DM, et al. Maintenance of human hepatocyte function in vitro by liver-derived extracellular matrix gels. Article. Tissue Eng Part A. 2010;16(3):1075-1082.
doi: 10.1089/ten.tea.2008.0587
71.Sutherland AJ, Converse GL, Hopkins RA, Detamore MS. The bioactivity of cartilage extracellular matrix in articular cartilage regeneration. Review. Adv Healthc Mater. 2015;4(1):29-39.
72.Brown M, Li J, Moraes C, Tabrizian M, Li-Jessen NYK. Decellularized extracellular matrix: new promising and challenging biomaterials for regenerative medicine. Article. Biomaterials. 2022;289:121786.
doi: 10.1016/j.biomaterials.2022.121786
73.Liu C, Jin Z, Ge X, Zhang Y, Xu H. Decellularized annulus fibrosus matrix/chitosan hybrid hydrogels with basic fibroblast growth factor for annulus fibrosus tissue engineering. Article. Tissue Eng Part A. 2019;25(23-24):1605-1613.
doi: 10.1089/ten.tea.2018.0297
74.Franc S, Rousseau JC, Garrone R, van der Rest M, Moradi-Améli M. Microfibrillar composition of umbilical cord matrix: characterization of fibrillin, collagen VI and intact collagen V. Placenta. 1998;19(1):95-104.
doi: 10.1016/s0143-4004(98)90104-7
75.Sobolewski K, Małkowski A, Bańkowski E, Jaworski S. Wharton’s jelly as a reservoir of peptide growth factors. Placenta. 2005;26(10):747-752.
doi: 10.1016/j.placenta.2004.10.008
76.Xiao T, Guo W, Chen M, et al. Fabrication and in vitro study of tissue-engineered cartilage scaffold derived from Wharton’s jelly extracellular matrix. Biomed Res Int. 2017;2017:5839071.
doi: 10.1155/2017/5839071
77.Valot L, Martinez J, Mehdi A, Subra G. Chemical insights into bioinks for 3D printing. Review. Chem Soc Rev. 2019;48(15):4049-4086.
doi: 10.1039/c7cs00718c
78.Gopinathan J, Noh I. Recent trends in bioinks for 3D printing. Review. Biomater Res. 2018;22:11-11.
doi: 10.1186/s40824-018-0122-1
79.Lin C-C, Anseth KS. PEG hydrogels for the controlled release of biomolecules in regenerative medicine. Review. Pharm Res. 2009;26(3):631-643.
doi: 10.1007/s11095-008-9801-2
80.Cui X, Li J, Hartanto Y, et al. Advances in extrusion 3D bioprinting: a focus on multicomponent hydrogel-based bioinks. Review. Adv Healthc Mater. 2020;9(15): 1901648.
81.Wolberg AS. Thrombin generation and fibrin clot structure. Blood Rev. 2007;21(3):131-142.
doi: 10.1016/j.blre.2006.11.001
82.Piechocka IK, Kurniawan NA, Grimbergen J, Koopman J, Koenderink GH. Recombinant fibrinogen reveals the differential roles of α- and γ-chain cross-linking and molecular heterogeneity in fibrin clot strain-stiffening. J Thromb Haemost. 2017;15(5):938-949.
doi: 10.1111/jth.13650
83.de Melo BAG, Jodat YA, Cruz EM, Benincasa JC, Shin SR, Porcionatto MA. Strategies to use fibrinogen as bioink for 3D bioprinting fibrin-based soft and hard tissues. Acta Biomater. 2020;117:60-76.
doi: 10.1016/j.actbio.2020.09.024
84.Chiu CL, Hecht V, Duong H, Wu B, Tawil B. Permeability of three-dimensional fibrin constructs corresponds to fibrinogen and thrombin concentrations. Biores Open Access. 2012;1(1):34-40.
85.Duong H, Wu B, Tawil B. Modulation of 3D fibrin matrix stiffness by intrinsic fibrinogen-thrombin compositions and by extrinsic cellular activity. Tissue Eng Part A. 2009;15(7):1865-1876.
doi: 10.1089/ten.tea.2008.0319
86.Snyder TN, Madhavan K, Intrator M, Dregalla RC, Park D. A fibrin/hyaluronic acid hydrogel for the delivery of mesenchymal stem cells and potential for articular cartilage repair. J Biol Eng. 2014;8:10.
87.Arulmoli J, Wright HJ, Phan DTT, et al. Combination scaffolds of salmon fibrin, hyaluronic acid, and laminin for human neural stem cell and vascular tissue engineering. Acta Biomater. 2016;43:122-138.
doi: 10.1016/j.actbio.2016.07.043
88.Singaravelu S, Ramanathan G, Raja MD, et al. Biomimetic interconnected porous keratin-fibrin-gelatin 3D sponge for tissue engineering application. Int J Biol Macromol. 2016;86:810-819.
doi: 10.1016/j.ijbiomac.2016.02.021
89.Deepthi S, Jayakumar R. Alginate nanobeads interspersed fibrin network as in situ forming hydrogel for soft tissue engineering. Bioact Mater. 2018;3(2):194-200.
doi: 10.1016/j.bioactmat.2017.09.005
90.Cui X, Boland T. Human microvasculature fabrication using thermal inkjet printing technology. Biomaterials. 2009;30(31):6221-6227.
doi: 10.1016/j.biomaterials.2009.07.056
91.de Melo BAG, Jodat YA, Mehrotra S, et al. 3D printed cartilage-like tissue constructs with spatially controlled mechanical properties. Adv Funct Mater. 2019;29(51).
92.Tang-Schomer MD, White JD, Tien LW, et al. Bioengineered functional brain-like cortical tissue. Proc Natl Acad Sci U S A. 2014;111(38):13811-13816.
93.Anil Kumar S, Alonzo M, Allen SC, et al. A visible light-cross-linkable, fibrin-gelatin-based bioprinted construct with human cardiomyocytes and fibroblasts. ACS Biomater Sci Eng. 2019;5(9):4551-4563.
doi: 10.1021/acsbiomaterials.9b00505
94.Cubo N, Garcia M, Del Cañizo JF, Velasco D, Jorcano JL. 3D bioprinting of functional human skin: production and in vivo analysis. Biofabrication. 2016;9(1):015006.
doi: 10.1088/1758-5090/9/1/015006
95.Costantini M, Testa S, Mozetic P, et al. Microfluidic-enhanced 3D bioprinting of aligned myoblast-laden hydrogels leads to functionally organized myofibers in vitro and in vivo. Biomaterials. 2017;131:98-110.
doi: 10.1016/j.biomaterials.2017.03.026
96.de la Vega L, Gomez DAR, Abelseth E, Abelseth L, da Silva VA, Willerth SM. 3D bioprinting human induced pluripotent stem cell-derived neural tissues using a novel lab-on-a-printer technology. Appl Sci-Basel. 2018;8(12):2414.
doi: 10.3390/app8122414
97.Kang HW, Lee SJ, Ko IK, Kengla C, Yoo JJ, Atala A. A 3D bioprinting system to produce human-scale tissue constructs with structural integrity. Nat Biotechnol. 2016;34(3):312-319.
doi: 10.1038/nbt.3413
98.Phillippi JA, Miller E, Weiss L, Huard J, Waggoner A, Campbell P. Microenvironments engineered by inkjet bioprinting spatially direct adult stem cells toward muscle- and bone-like subpopulations. Stem Cells. 2008;26(1):127-134.
doi: 10.1634/stemcells.2007-0520
99.Crecente-Campo J, Borrajo E, Vidal A, Garcia-Fuentes M. New scaffolds encapsulating TGF-beta 3/BMP-7 combinations driving strong chondrogenic differentiation. Article. Eur J Pharm Biopharm. 2017;114:69-78.
doi: 10.1016/j.ejpb.2016.12.021
100.Liu F, Wang X. Synthetic polymers for organ 3D printing. Review. Polymers. 2020;12(8):1765.
101.Wu W, DeConinck A, Lewis JA. Omnidirectional printing of 3D microvascular networks. Article. Adv Mater. 2011;23(24):H178-H183.
102.Zhu J. Bioactive modification of poly(ethylene glycol) hydrogels for tissue engineering. Review. Biomaterials. 2010;31(17):4639-4656.
doi: 10.1016/j.biomaterials.2010.02.044
103.Serra T, Ortiz-Hernandez M, Engel E, Planell JA, Navarro M. Relevance of PEG in PLA-based blends for tissue engineering 3D-printed scaffolds. Article. Mater Sci Eng C-Mater Biol Appl. 2014;38:55-62.
doi: 10.1016/j.msec.2014.01.003
104.Rutz AL, Hyland KE, Jakus AE, Burghardt WR, Shah RN. A multimaterial bioink method for 3D printing tunable, cell-compatible hydrogels. Article. Adv Mater. 2015;27(9):1607-1614.
105.Mukherjee P, Chung J, Cheng K, et al. In vitro and In vivo study of PCL-hydrogel scaffold to advance bioprinting translation in microtia reconstruction. Article. J Craniofac Surg. 2021;32(5):1931-1936.
doi: 10.1097/scs.0000000000007173
106.Daly AC, Critchley SE, Rencsok EM, Kelly DJ. A comparison of different bioinks for 3D bioprinting of fibrocartilage and hyaline cartilage. Article. Biofabrication. 2016; 8(4):045002.
doi: 10.1088/1758-5090/8/4/045002
107.Singhvi MS, Zinjarde SS, Gokhale DV. Polylactic acid: synthesis and biomedical applications. Review. J Appl Microbiol. 2019;127(6):1612-1626.
doi: 10.1111/jam.14290
108.Ritz U, Gerke R, Goetz H, Stein S, Rommens PM. A new bone substitute developed from 3D-prints of polylactide (PLA) loaded with collagen I: an in vitro study. Article. Int J Mol Sci. 2017;18(12):2569.
doi: 10.3390/ijms18122569
109.Graf N, Bielenberg DR, Kolishetti N, et al. Alpha(V)beta(3) integrin-targeted PLGA-PEG nanoparticles for enhanced anti-tumor efficacy of a Pt(IV) prodrug. Article. ACS Nano. 2012;6(5):4530-4539.
doi: 10.1021/nn301148e
110.Jin S, Xia X, Huang J, et al. Recent advances in PLGA-based biomaterials for bone tissue regeneration. Review. Acta Biomater. 2021;127:56-79.
doi: 10.1016/j.actbio.2021.03.067
111.Chang CC, Boland ED, Williams SK, Hoying JB. Direct-write bioprinting three-dimensional biohybrid systems for future regenerative therapies. Review. J Biomed Mater Res Part B Appl Biomater. 2011;98B(1):160-170.
doi: 10.1002/jbm.b.31831
112.Mueller M, Becher J, Schnabelrauch M, Zenobi-Wong M. Nanostructured pluronic hydrogels as bioinks for 3D bioprinting. Article. Biofabrication. 2015;7(3):035006.
doi: 10.1088/1758-5090/7/3/035006
113.Madry H, Gao L, Rey-Rico A, et al. Thermosensitive hydrogel based on PEO-PPO-PEO poloxamers for a controlled in situ release of recombinant adeno-associated viral vectors for effective gene therapy of cartilage defects. Article. Adv Mater. 2020;32(2):1906508.
114.Nakanishi W, Minami K, Shrestha LK, Ji Q, Hill JP, Ariga K. Bioactive nanocarbon assemblies: Nanoarchitectonics and applications. Review. Nano Today. 2014;9(3):378-394.
doi: 10.1016/j.nantod.2014.05.002
115.Saifuddin N, Raziah AZ, Junizah AR. Carbon nanotubes: a review on structure and their interaction with proteins. Review. J Chem. 2013;2013:676815.
doi: 10.1155/2013/676815
116.Tanaka M, Sato Y, Zhang M, et al. In vitro and in vivo evaluation of a three-dimensional porous multi-walled carbon nanotube scaffold for bone regeneration. Nanomaterials (Basel). 2017;7(2).
doi: 10.3390/nano7020046
117.Usui Y, Aoki K, Narita N, et al. Carbon nanotubes with high bone-tissue compatibility and bone-formation acceleration effects. Small. 2008;4(2):240-246.
118.Shimizu M, Kobayashi Y, Mizoguchi T, etal. Carbon nanotubes induce bone calcification by bidirectional interaction with osteoblasts. Adv Mater. 2012;24(16):2176-2185.
119.Trzeciak T, Rybka JD, Akinoglu EM, Richter M, Kaczmarczyk J, Giersig M. In vitro evaluation of carbon nanotube-based scaffolds for cartilage tissue engineering. Article. J Nanosci Nanotechnol. 2016;16(9):9022-9025.
120.Szymański T, Mieloch AA, Richter M, et al. Utilization of carbon nanotubes in manufacturing of 3D cartilage and bone scaffolds. Materials (Basel). 2020;13(18):4039.
doi: 10.3390/ma13184039
121.Stocco TD, Moreira Silva MC, Corat MAF, Gonçalves Lima G, Lobo AO. Towards bioinspired meniscus-regenerative scaffolds: engineering a novel 3D bioprinted patient-specific construct reinforced by biomimetically aligned nanofibers. Int J Nanomed. 2022;17:1111-1124.
doi: 10.2147/ijn.S353937
122.Qu H, Fu H, Han Z, Sun Y. Biomaterials for bone tissue engineering scaffolds: a review. RSC Adv. 2019;9(45):26252-26262.
doi: 10.1039/c9ra05214c
123.Du Z, Feng X, Cao G, et al. The effect of carbon nanotubes on osteogenic functions of adipose-derived mesenchymal stem cells in vitro and bone formation in vivo compared with that of nano-hydroxyapatite and the possible mechanism. Bioact Mater. 2021;6(2):333-345.
doi: 10.1016/j.bioactmat.2020.08.015
124.Wang W, Huang B, Byun JJ, Bártolo P. Assessment of PCL/carbon material scaffolds for bone regeneration. J Mech Behav Biomed Mater. 2019;93:52-60.
doi: 10.1016/j.jmbbm.2019.01.020
125.Gonçalves EM, Oliveira FJ, Silva RF, et al. Three-dimensional printed PCL-hydroxyapatite scaffolds filled with CNTs for bone cell growth stimulation. J Biomed Mater Res B Appl Biomater. 2016;104(6):1210-1219.
doi: 10.1002/jbm.b.33432
126.Chahine NO, Collette NM, Thomas CB, Genetos DC, Loots GG. Nanocomposite scaffold for chondrocyte growth and cartilage tissue engineering: effects of carbon nanotube surface functionalization. Tissue Eng Part A. 2014;20(17-18):2305-2315.
doi: 10.1089/ten.TEA.2013.0328
127.Deligianni DD. Multiwalled carbon nanotubes enhance human bone marrow mesenchymal stem cells’ spreading but delay their proliferation in the direction of differentiation acceleration. Editorial Material. Cell Adh Migr. 2014;8(6):558-562.
doi: 10.4161/cam.32124
128.Castranova V, Schulte PA, Zumwalde RD. Occupational nanosafety considerations for carbon nanotubes and carbon nanofibers. Acc Chem Res. 2013;46(3):642-649.
doi: 10.1021/ar300004a
129.Aldieri E, Fenoglio I, Cesano F, et al. The role of iron impurities in the toxic effects exerted by short multiwalled carbon nanotubes (MWCNT) in murine alveolar macrophages. J Toxicol Environ Health A. 2013;76(18):1056-1071.
doi: 10.1080/15287394.2013.834855
130.Moon RJ, Martini A, Nairn J, Simonsen J, Youngblood J. Cellulose nanomaterials review: structure, properties and nanocomposites. Chem Soc Rev. 2011;40(7):3941-3994.
doi: 10.1039/c0cs00108b
131.Ferreira PJT, Lourenço AF. Nanocelluloses: production, characterization and market. Adv Exp Med Biol. 2022;1357:129-151.
doi: 10.1007/978-3-030-88071-2_6
132.Yang J, Han CR, Duan JF, Xu F, Sun RC. Mechanical and viscoelastic properties of cellulose nanocrystals reinforced poly(ethylene glycol) nanocomposite hydrogels. ACS Appl Mater Interfaces. 2013;5(8):3199-3207.
doi: 10.1021/am4001997
133.Cui Y, Jin R, Zhang Y, Yu M, Zhou Y, Wang LQ. Cellulose nanocrystal-enhanced thermal-sensitive hydrogels of block copolymers for 3D bioprinting. Int J Bioprint. 2021;7(4):397.
134.Liu M, Zhang Y, Wu C, Xiong S, Zhou C. Chitosan/halloysite nanotubes bionanocomposites: structure, mechanical properties and biocompatibility. Int J Biol Macromol. 2012;51(4):566-575.
doi: 10.1016/j.ijbiomac.2012.06.022
135.Liu M, Dai L, Shi H, Xiong S, Zhou C. In vitro evaluation of alginate/halloysite nanotube composite scaffolds for tissue engineering. Mater Sci Eng C Mater Biol Appl. 2015;49:700-712.
doi: 10.1016/j.msec.2015.01.037
136.Huang B, Liu M, Long Z, Shen Y, Zhou C. Effects of halloysite nanotubes on physical properties and cytocompatibility of alginate composite hydrogels. Mater Sci Eng C Mater Biol Appl. 2017;70(Pt 1):303-310.
doi: 10.1016/j.msec.2016.09.001
137.Roushangar Zineh B, Shabgard MR, Roshangar L. An experimental study on the mechanical and biological properties of bio-printed alginate/halloysite nanotube/methylcellulose/Russian olive-based scaffolds. Adv Pharm Bull. 2018;8(4):643-655.
138.Chakraborty J, Fernández-Pérez J, van Kampen KA, et al. Development of a biomimetic arch-like 3D bioprinted construct for cartilage regeneration using gelatin methacryloyl and silk fibroin-gelatin bioinks. Biofabrication. 2023;15(3).
139.Flégeau K, Puiggali-Jou A, Zenobi-Wong M. Cartilage tissue engineering by extrusion bioprinting utilizing porous hyaluronic acid microgel bioinks. Biofabrication. 2022;14(3).
140.Gorroñogoitia I, Urtaza U, Zubiarrain-Laserna A, Alonso-Varona A, Zaldua AM. A study of the printability of alginate-based bioinks by 3D bioprinting for articular cartilage tissue engineering. Polymers (Basel). 2022;14(2):354.
141.Zhao J, Qiu P, Wang Y, et al. Chitosan-based hydrogel wound dressing: From mechanism to applications, a review. Int J Biol Macromol. 2023;244:125250.
doi: 10.1016/j.ijbiomac.2023.125250
142.Kim BS, Das S, Jang J, Cho DW. Decellularized extracellular matrix-based bioinks for engineering tissue- and organ-specific microenvironments. Chem Rev. 2020;120(19):10608-10661.
doi: 10.1021/acs.chemrev.9b00808
143.Simińska-Stanny J, Nicolas L, Chafai A, et al. Advanced PEG-tyramine biomaterial ink for precision engineering of perfusable and flexible small-diameter vascular constructs via coaxial printing. Bioact Mater. 2024;36:168-184.
doi: 10.1016/j.bioactmat.2024.02.019
144.Alizadeh Sardroud H, Chen X, Eames BF. Reinforcement of hydrogels with a 3D-printed polycaprolactone (PCL) structure enhances cell numbers and cartilage ECM production under compression. J Funct Biomater. 2023;14(6):313.
doi: 10.3390/jfb14060313
145.Brézulier D, Chaigneau L, Jeanne S, Lebullenger R. The challenge of 3D bioprinting of composite natural polymers PLA/bioglass: trends and benefits in cleft palate surgery. Biomedicines. 2021;9(11):1553.
doi: 10.3390/biomedicines9111553
146.Couto M, Vasconcelos DP, Pereira CL, Neto E, Sarmento B, Lamghari M. Neuro-immunomodulatory potential of nanoenabled 4D bioprinted microtissue for cartilage tissue engineering. Adv Healthc Mater. 2025;14(5):e2400496.
147.Moncal KK, Ozbolat V, Datta P, Heo DN, Ozbolat IT. Thermally-controlled extrusion-based bioprinting of collagen. J Mater Sci Mater Med. 2019;30(5):55.
doi: 10.1007/s10856-019-6258-2
148.Kim SA, Lee Y, Park K, et al. 3D printing of mechanically tough and self-healing hydrogels with carbon nanotube fillers. Int J Bioprint. 2023;9(5):765.
doi: 10.18063/ijb.765
149.Buckwalter JA, Mankin HJ. Articular cartilage: tissue design and chondrocyte-matrix interactions. Instr Course Lect. 1998;47:477-486.
150.Bullough PG, Jagannath A. The morphology of the calcification front in articular cartilage. Its significance in joint function. J Bone Joint Surg Br Vol. 1983;65(1):72-78.
doi: 10.1302/0301-620x.65b1.6337169
151.Yang J, Zhang YS, Yue K, Khademhosseini A. Cell-laden hydrogels for osteochondral and cartilage tissue engineering. Acta Biomater. 2017;57:1-25.
doi: 10.1016/j.actbio.2017.01.036
152.Carballo CB, Nakagawa Y, Sekiya I, Rodeo SA. Basic science of articular cartilage. Clin Sports Med. 2017;36(3):413-425.
doi: 10.1016/j.csm.2017.02.001
153.Duarte Campos DF, Drescher W, Rath B, Tingart M, Fischer H. Supporting biomaterials for articular cartilage repair. Cartilage. 2012;3(3):205-221.
154.Liao IC, Moutos FT, Estes BT, Zhao X, Guilak F. Composite three-dimensional woven scaffolds with interpenetrating network hydrogels to create functional synthetic articular cartilage. Adv Funct Mater. 2013;23(47):5833-5839.
155.Shin H, Olsen BD, Khademhosseini A. The mechanical properties and cytotoxicity of cell-laden double-network hydrogels based on photocrosslinkable gelatin and gellan gum biomacromolecules. Biomaterials. 2012;33(11):3143-3152.
doi: 10.1016/j.biomaterials.2011.12.050
156.Krüger R, Groll J. Fiber reinforced calcium phosphate cements—on the way to degradable load bearing bone substitutes? Biomaterials. 2012;33(25):5887-5900.
doi: 10.1016/j.biomaterials.2012.04.053
157.Schipani R, Scheurer S, Florentin R, Critchley SE, Kelly DJ. Reinforcing interpenetrating network hydrogels with 3D printed polymer networks to engineer cartilage mimetic composites. Biofabrication. 2020;12(3):035011.
158.Boere KW, Visser J, Seyednejad H, et al. Covalent attachment of a three-dimensionally printed thermoplast to a gelatin hydrogel for mechanically enhanced cartilage constructs. Acta Biomater. 2014;10(6):2602-2611.
doi: 10.1016/j.actbio.2014.02.041
159.Sivashankari PR, Prabaharan M. Three-dimensional porous scaffolds based on agarose/chitosan/graphene oxide composite for tissue engineering. Int J Biol Macromol. 2020;146:222-231.
doi: 10.1016/j.ijbiomac.2019.12.219
160.Ghiasi B, Sefidbakht Y, Mozaffari-Jovin S, et al. Hydroxyapatite as a biomaterial—a gift that keeps on giving. Drug Dev Ind Pharm. 2020;46(7):1035-1062.
doi: 10.1080/03639045.2020.1776321
161.Huang J, Huang Z, Liang Y, et al. 3D printed gelatin/hydroxyapatite scaffolds for stem cell chondrogenic differentiation and articular cartilage repair. Biomater Sci. 2021;9(7):2620-2630.
doi: 10.1039/d0bm02103b
162.Cui X, Breitenkamp K, Lotz M, D’Lima D. Synergistic action of fibroblast growth factor-2 and transforming growth factor-beta1 enhances bioprinted human neocartilage formation. Biotechnol Bioeng. 2012;109(9):2357-2368.
doi: 10.1002/bit.24488
163.Hauptstein J, Forster L, Nadernezhad A, Groll J, Teßmar J, Blunk T. Tethered TGF-β1 in a hyaluronic acid-based bioink for bioprinting cartilaginous tissues. Int J Mol Sci. 2022;23(2):924.
doi: 10.3390/ijms23020924
164.Shi W, Fang F, Kong Y, et al. Dynamic hyaluronic acid hydrogel with covalent linked gelatin as an anti-oxidative bioink for cartilage tissue engineering. Biofabrication. 2021;14(1).
165.Mouser VHM, Levato R, Bonassar LJ, et al. Three-dimensional bioprinting and its potential in the field of articular cartilage regeneration. Cartilage. 2017;8(4):327-340.
166.Cui X, Breitenkamp K, Finn MG, Lotz M, D’Lima DD. Direct human cartilage repair using three-dimensional bioprinting technology. Tissue Eng Part A. 2012;18(11-12): 1304-1312.
doi: 10.1089/ten.TEA.2011.0543
167.Olate-Moya F, Arens L, Wilhelm M, Mateos-Timoneda MA, Engel E, Palza H. Chondroinductive alginate-based hydrogels having graphene oxide for 3D printed scaffold fabrication. ACS Appl Mater Interfaces. 2020;12(4):4343-4357.
168.Ni T, Liu M, Zhang Y, Cao Y, Pei R. 3D bioprinting of bone marrow mesenchymal stem cell-laden silk fibroin double network scaffolds for cartilage tissue repair. Bioconjug Chem. 2020;31(8):1938-1947.
doi: 10.1021/acs.bioconjchem.0c00298
169.Nedunchezian S, Banerjee P, Lee CY, et al. Generating adipose stem cell-laden hyaluronic acid-based scaffolds using 3D bioprinting via the double crosslinked strategy for chondrogenesis. Mater Sci Eng C Mater Biol Appl. 2021;124:112072.
doi: 10.1016/j.msec.2021.112072
170.Levato R, Webb WR, Otto IA, et al. The bio in the ink: cartilage regeneration with bioprintable hydrogels and articular cartilage-derived progenitor cells. Acta Biomater. 2017;61:41-53.
doi: 10.1016/j.actbio.2017.08.005
171.Xu Y, Peng J, Richards G, Lu S, Eglin D. Optimization of electrospray fabrication of stem cell-embedded alginate-gelatin microspheres and their assembly in 3D-printed poly(ε-caprolactone) scaffold for cartilage tissue engineering. J Orthop Translat. 2019;18:128-141.
doi: 10.1016/j.jot.2019.05.003
172.Duchi S, Onofrillo C, O’Connell CD, et al. Handheld co-axial bioprinting: application to in situ surgical cartilage repair. Sci Rep. 2017;7(1):5837.
doi: 10.1038/s41598-017-05699-x
173.Tamaddon M, Wang L, Liu Z, Liu C. Osteochondral tissue repair in osteoarthritic joints: clinical challenges and opportunities in tissue engineering. Biodes Manuf. 2018;1(2):101-114.
doi: 10.1007/s42242-018-0015-0
174.Radhakrishnan J, Subramanian A, Krishnan UM, Sethuraman S. Injectable and 3D bioprinted polysaccharide hydrogels: from cartilage to osteochondral tissue engineering. Biomacromolecules. 2017;18(1):1-26.
doi: 10.1021/acs.biomac.6b01619
175.Critchley S, Sheehy EJ, Cunniffe G, et al. 3D printing of fibre-reinforced cartilaginous templates for the regeneration of osteochondral defects. Acta Biomater. 2020;113:130-143.
doi: 10.1016/j.actbio.2020.05.040
176.Zhu S, Chen P, Chen Y, Li M, Chen C, Lu H. 3D-printed extracellular matrix/polyethylene glycol diacrylate hydrogel incorporating the anti-inflammatory phytomolecule honokiol for regeneration of osteochondral defects. Am J Sports Med. 2020;48(11):2808-2818.
177.Chen Y, Chen Y, Xiong X, et al. Hybridizing gellan/alginate and thixotropic magnesium phosphate-based hydrogel scaffolds for enhanced osteochondral repair. Mater Today Bio. 2022;14:100261.
doi: 10.1016/j.mtbio.2022.100261
178.Kilian D, Ahlfeld T, Akkineni AR, Bernhardt A, Gelinsky M, Lode A. 3D bioprinting of osteochondral tissue substitutes—in vitro-chondrogenesis in multi-layered mineralized constructs. Sci Rep. 2020;10(1):8277.
doi: 10.1038/s41598-020-65050-9
179.Nowicki MA, Castro NJ, Plesniak MW, Zhang LG. 3D printing of novel osteochondral scaffolds with graded microstructure. Nanotechnology. 2016;27(41):414001.
doi: 10.1088/0957-4484/27/41/414001
180.Du Y, Liu H, Yang Q, et al. Selective laser sintering scaffold with hierarchical architecture and gradient composition for osteochondral repair in rabbits. Biomaterials. 2017;137:37-48.
doi: 10.1016/j.biomaterials.2017.05.021
181.Hinton TJ, Jallerat Q, Palchesko RN, et al. Three-dimensional printing of complex biological structures by freeform reversible embedding of suspended hydrogels. Sci Adv. 2015;1(9):e1500758.
182.Jalandhra GK, Molley TG, Hung TT, Roohani I, Kilian KA. In situ formation of osteochondral interfaces through “bone-ink” printing in tailored microgel suspensions. Acta Biomater. 2023;156:75-87.
doi: 10.1016/j.actbio.2022.08.052
183.Muir H. The chondrocyte, architect of cartilage— biomechanics, structure, function and molecular-biology of cartilage matrix macromolecules. Review. Bioessays. 1995;17(12):1039-1048.
184.Hutchinson ID, Moran CJ, Potter HG, Warren RF, Rodeo SA. Restoration of the meniscus form and function. Article. Am J Sports Med. 2014;42(4):987-998.
185.Katz JN, Brophy RH, Chaisson CE, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. Article. New Engl J Med. 2013;368(18):1675-1684.
186.Perera K, Ivone R, Natekin E, Wilga CA, Shen J, Menon JU. 3D bioprinted implants for cartilage repair in intervertebral discs and knee menisci. Front Bioeng Biotechnol. 2021;9:754113.
doi: 10.3389/fbioe.2021.754113
187.Toh WS, Foldager CB, Pei M, Hui JHP. Advances in mesenchymal stem cell-based strategies for cartilage repair and regeneration. Article. Stem Cell Rev Rep. 2014;10(5):686-696.
doi: 10.1007/s12015-014-9526-z
188.Pereira H, Frias AM, Oliveira JM, Espregueira-Mendes J, Reis RL. Tissue engineering and regenerative medicine strategies in meniscus lesions. Review. Arthroscopy. 2011;27(12):1706-1719.
doi: 10.1016/j.arthro.2011.08.283
189.Zhang Y, Li P, Wang H, Wang Y, Song K, Liu T. Research progress on reconstruction of meniscus in tissue engineering. Article. J Sports Med Phys Fitness. 2017;57(5):595-603.
doi: 10.23736/s0022-4707.16.06378-7
190.Stocco E, Porzionato A, De Rose E, Barbon S, De Caro R, Macchi V. Meniscus regeneration by 3D printing technologies: current advances and future perspectives. Review. J Tissue Eng. 2022;13:20417314211065860.
doi: 10.1177/20417314211065860
191.Bahcecioglu G, Bilgen B, Hasirci N, Hasirci V. Anatomical meniscus construct with zone specific biochemical composition and structural organization. Article. Biomaterials. 2019;218:119361.
doi: 10.1016/j.biomaterials.2019.119361
192.van Uden S, Silva-Correia J, Oliveira JM, Reis RL. Current strategies for treatment of intervertebral disc degeneration: substitution and regeneration possibilities. Review. Biomater Res. 2017;21:22-22.
doi: 10.1186/s40824-017-0106-6
193.De Pieri A, Byerley AM, Musumeci CR, Salemizadehparizi F, Vanderhorst MA, Wuertz-Kozak K. Electrospinning and 3D bioprinting for intervertebral disc tissue engineering. Review. JOR Spine. 2020;3(4)e1117.
doi: 10.1002/jsp2.1117
194.Frost BA, Camarero-Espinosa S, Foster EJ. Materials for the spine: anatomy, problems, and solutions. Review. Materials. 2019;12(2):253.
doi: 10.3390/ma12020253
195.Hu D, Wu D, Huang L, et al. 3D bioprinting of cell-laden scaffolds for intervertebral disc regeneration. Article. Mater Lett 2018;223:219-222.
doi: 10.1016/j.matlet.2018.03.204
196.Chen Q, Chen H, Zhu L, Zheng J. Fundamentals of double network hydrogels. Review. J Mater Chem B. 2015;3(18):3654-3676.
doi: 10.1039/c5tb00123d
197.Moxon SR, McMurran Z, Kibble MJ, Domingos M, Gough JE, Richardson SM. 3D bioprinting of an intervertebral disc tissue analogue with a highly aligned annulus fibrosus via suspended layer additive manufacture. Biofabrication. 2024;17(1).
198.Sun B, Lian M, Han Y, et al. A 3D-bioprinted dual growth factor-releasing intervertebral disc scaffold induces nucleus pulposus and annulus fibrosus reconstruction. Bioact Mater. 2021;6(1):179-190.
doi: 10.1016/j.bioactmat.2020.06.022
199.Storck K, Staudenmaier R, Buchberger M, et al. Total reconstruction of the auricle: our experiences on indications and recent techniques. Review. Biomed Res Int. 2014;2014:373286.
doi: 10.1155/2014/373286
200.Nayyer L, Patel KH, Esmaeili A, et al. Tissue engineering: revolution and challenge in auricular cartilagere construction. Article. Plast Reconstr Surg. 2012;129(5):1123-1137.
doi: 10.1097/PRS.0b013e31824a2c1c
201.Bhamare N, Tardalkar K, Parulekar P, Khadilkar A, Joshi M. 3D printing of human ear pinna using cartilage specific ink. Article. Biomed Mater. 2021;16(5):055008.
202.Cao YL, Vacanti JP, Paige KT, Upton J, Vacanti CA. Transplantation of chondrocytes utilizing a polymer-cell construct to produce tissue-engineered cartilage in the shape of a human ear. Article. Proceedings paper. Plast Reconstr Surg. 1997;100(2):297-302.
doi: 10.1097/00006534-199708000-00001
203.Di Gesu R, Acharya AP, Jacobs I, Gottardi R. 3D printing for tissue engineering in otolaryngology. Article. Connect Tissue Res. 2020;61(2):117-136.
doi: 10.1080/03008207.2019.1663837
204.Tollefson TT. Advances in the treatment of microtia. Review. Curr Opin Otolaryngol Head Neck Surg. 2006;14(6):412-422.
doi: 10.1097/MOO.0b013e328010633a
205.Mussi E, Furferi R, Volpe Y, Facchini F, McGreevy KS, Uccheddu F. Ear reconstruction simulation: from handcrafting to 3D printing. Review. Bioengineering-Basel. 2019;6(1):14.
doi: 10.3390/bioengineering6010014
206.Pham TB, Sah RL, Masuda K, Watson D. Human septal cartilage tissue engineering: current methodologies and future directions. Bioengineering (Basel, Switzerland). 2024;11(11):1123.
doi: 10.3390/bioengineering11111123
207.Watson D, Reuther MS. Tissue-engineered cartilage for facial plastic surgery. Curr Opin Otolaryngol Head Neck Surg. 2014;22(4):300-306.
doi: 10.1097/moo.0000000000000068
208.Bagher Z, Asgari N, Bozorgmehr P, Kamrava SK, Alizadeh R, Seifalian A. Will tissue-engineering strategies bring new hope for the reconstruction of nasal septal cartilage? Curr Stem Cell Res Ther. 2020;15(2):144-154.
doi: 10.2174/1574888x14666191212160757
209.Shokri A, Ramezani K, Jamalpour MR, et al. In vivo efficacy of 3D-printed elastin-gelatin-hyaluronic acid scaffolds for regeneration of nasal septal cartilage defects. J Biomed Mater Res Part B Appl Biomater. 2022;110(3):614-624.
doi: 10.1002/jbm.b.34940
210.Lan X, Liang Y, Erkut EJN, et al. Bioprinting of human nasoseptal chondrocytes-laden collagen hydrogel for cartilage tissue engineering. FASEB J. 2021;35(3):e21191.
211.Lan X, Liang Y, Vyhlidal M, et al. In vitro maturation and in vivo stability of bioprinted human nasal cartilage. J Tissue Eng. 2022;13:20417314221086368.
doi: 10.1177/20417314221086368
212.Choi JR, Yong KW, Choi JY. Effects of mechanical loading on human mesenchymal stem cells for cartilage tissue engineering. J Cell Physiol. 2018;233(3):1913-1928.
doi: 10.1002/jcp.26018
213.Wan H, Xiang J, Mao G, Pan S, Li B, Lu Y. Recent advances in the application of 3D-printing bioinks based on decellularized extracellular matrix in tissue engineering. ACS Omega. 2024;9(23):24219-24235.
214.Faramarzi N, Yazdi IK, Nabavinia M, et al. Patient-specific bioinks for 3D bioprinting of tissue engineering scaffolds. Adv Healthc Mater. 2018;7(11):e1701347.
215.Liu W, Zhang YS, Heinrich MA, et al. Rapid continuous multimaterial extrusion bioprinting. Adv Mater (Deerfield Beach, Fla). 2017;29(3).
216.Miri AK, Nieto D, Iglesias L, et al. Microfluidics-enabled multimaterial maskless stereolithographic bioprinting. Adv Mater (Deerfield Beach, Fla). 2018;30(27):e1800242.