

Melanoma outcomes in resource-limited oncology systems: Lessons from Albania in the era of global cancer health disparities

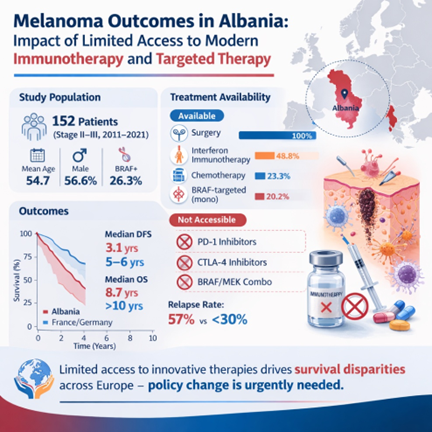
The rapid introduction of checkpoint inhibitors and BRAF/MEK-targeted therapies has transformed melanoma into one of oncology’s most curable malignancies. However, access to these agents remains profoundly unequal across regions. This study evaluates treatment outcomes for patients with non-metastatic melanoma (NMM) in Albania over a decade, highlighting how limited access to innovative treatments constrains survival improvements compared to Western European nations such as France and Germany. A retrospective analysis was conducted of 152 Albanian patients with NMM treated between 2011 and 2021 at the University Hospital Mother Theresa. Demographic, clinical, and therapeutic variables were extracted from medical records. Patients receiving surgery plus adjuvant or systemic therapy were included. Outcomes included overall survival (OS), disease-free survival (DFS), and relapse rates. BRAF mutation was present in 26.3% of patients. All patients underwent surgery; 84.9% received adjuvant systemic therapy. The predominant regimen was interferon-based immunotherapy (48.8%), followed by chemotherapy (23.3%) and targeted therapy (20.2%). No patients received checkpoint inhibitors during the study period, as anti-CTLA-4 and anti-PD-1 therapies were not approved in Albania. Relapse occurred in 57.2% of patients, with a mean relapse time of 1.6 years. Median DFS was 3.1 years and median OS 8.7 years, with a 10-year OS rate of 86.8%. Compared with published European data, Albanian patients experienced shorter DFS (3.1 vs. 5–6 years) and higher relapse rates, consistent with limited access to modern therapies. This study illustrates how systemic inequities in drug access perpetuate survival disparities across Europe. Thus, policies enabling equitable access to innovative cancer treatments are essential to translate scientific progress into population-level benefit.
- Arnold M, Singh D, Laversanne M, et al. Global Burden of Cutaneous Melanoma in 2020 and Projections to 2040. JAMA Dermatol. 2022;158(5):495-503. doi: 10.1001/jamadermatol.2022.0160
- Long GV, Hauschild A, Santinami M, et al. Adjuvant Dabrafenib plus Trametinib in Stage III BRAF-Mutated Melanoma. N Engl J Med. 2017;377(19):1813-1823. doi: 10.1056/NEJMoa1708539
- Eggermont AMM, Blank CU, Mandala M, et al. Adjuvant Pembrolizumab versus Placebo in Resected Stage III Melanoma. N Engl J Med. 2018;378(19):1789-1801. doi: 10.1056/NEJMoa1802357
- Weber J, Mandala M, Del Vecchio M, et al. Adjuvant Nivolumab versus Ipilimumab in Resected Stage III or IV Melanoma. N Engl J Med. 2017;377(19):1824-1835. doi: 10.1056/NEJMoa1709030
- Rueth NM, Groth SS, Tuttle TM, Virnig BA, Al-Refaie WB, Habermann EB. Conditional survival after surgical treatment of melanoma: an analysis of the Surveillance, Epidemiology, and End Results database. Ann Surg Oncol. 2010;17(6):1662-1668. doi: 10.1245/s10434-010-0965-8
- INCa (Institut National du Cancer). (n.d.). Les cancers en France – Édition 2021. Available from: https://www.cancer. fr/registre-national-des-cancers [Last accessed on]. [in French].
- Robert Koch Institute. (n.d.). Cancer in Germany 2017/2018. Available from: https://www.krebsdaten.de/Krebs/DE/ Home/homepage_node.html [Last accessed on].
- Ventola CL. Cancer Immunotherapy, Part 2: Efficacy, Safety, and Other Clinical Considerations. P T. 2017;42(7):452- 463. Available from: https://pmc.ncbi.nlm.nih.gov/articles/ PMC5481296/ [Last accessed on].
- Mela A, Rdzanek E, Tysarowski A, et al. The impact of changing the funding model for genetic diagnostics and improved access to personalized medicine in oncology. Expert Rev Pharm Outcomes Res. 2023;23(1):43-54. doi: 10.1080/14737167.2023.2140139